Understanding Urethroplasty
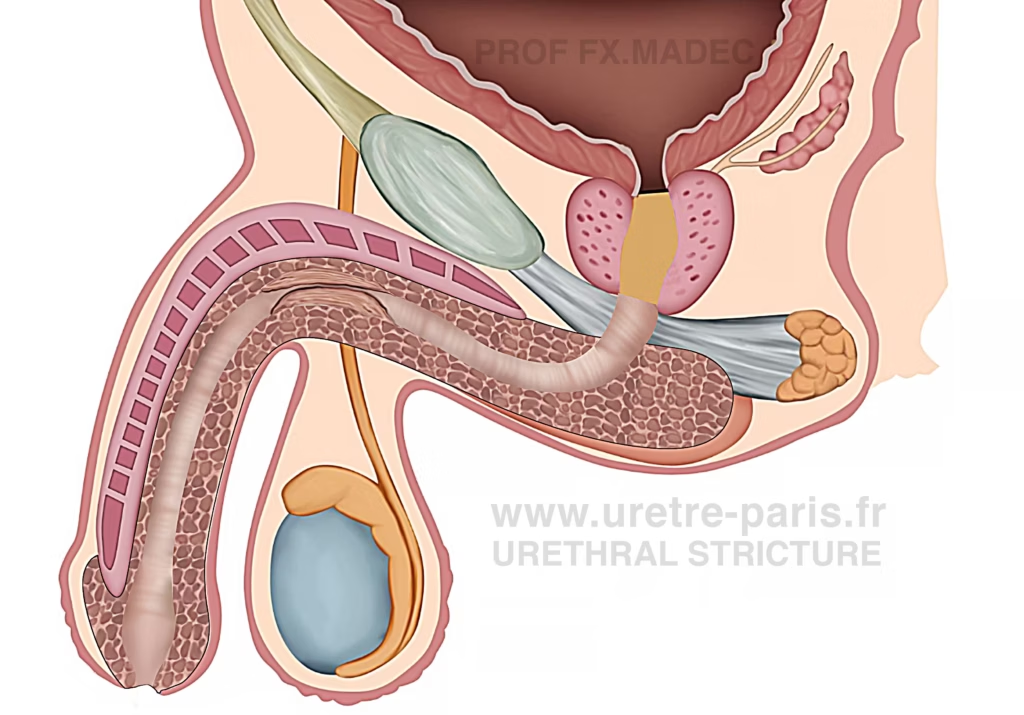
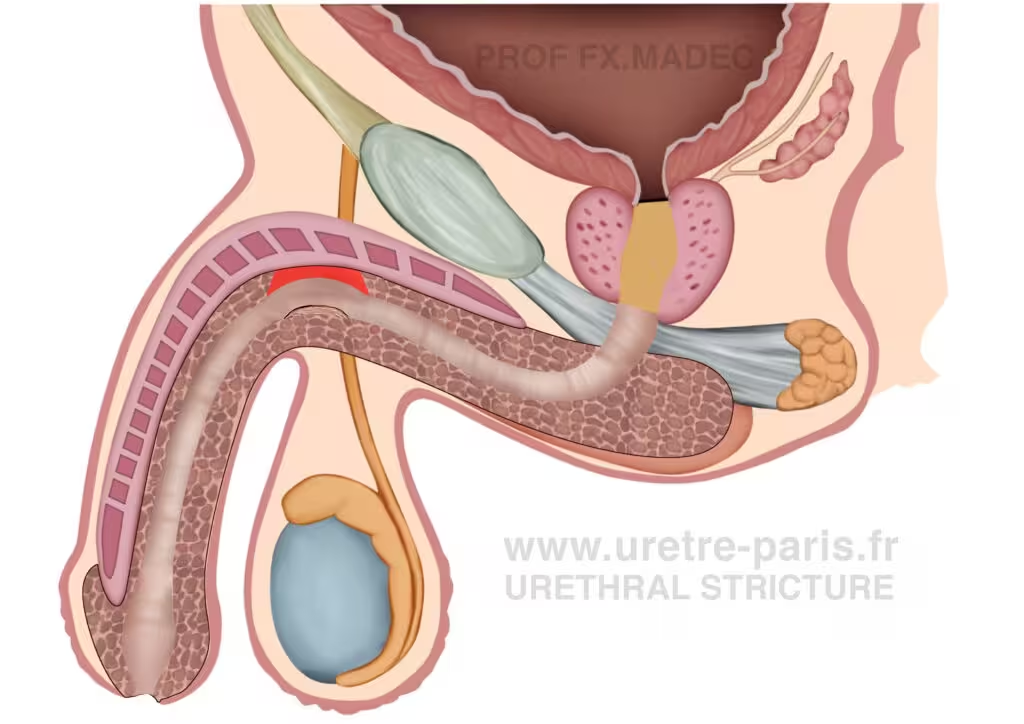
Urethroplasty is an open surgical procedure performed to repair a urethral stricture by removing or opening the narrowed, scarred segment of the urinary channel and reconstructing it either by direct suturing or by using another tissue when needed. Two main principles exist: anastomotic urethroplasty and substitution urethroplasty, using grafts or flaps. Over the past decade, urethroplasty has become the reference treatment for urethral stricture disease in most clinical situations. This evolution has been consistently reflected in national and international recommendations, including American, French, and European urethral stricture guidelines.
French Urethral Stricture Guidelines
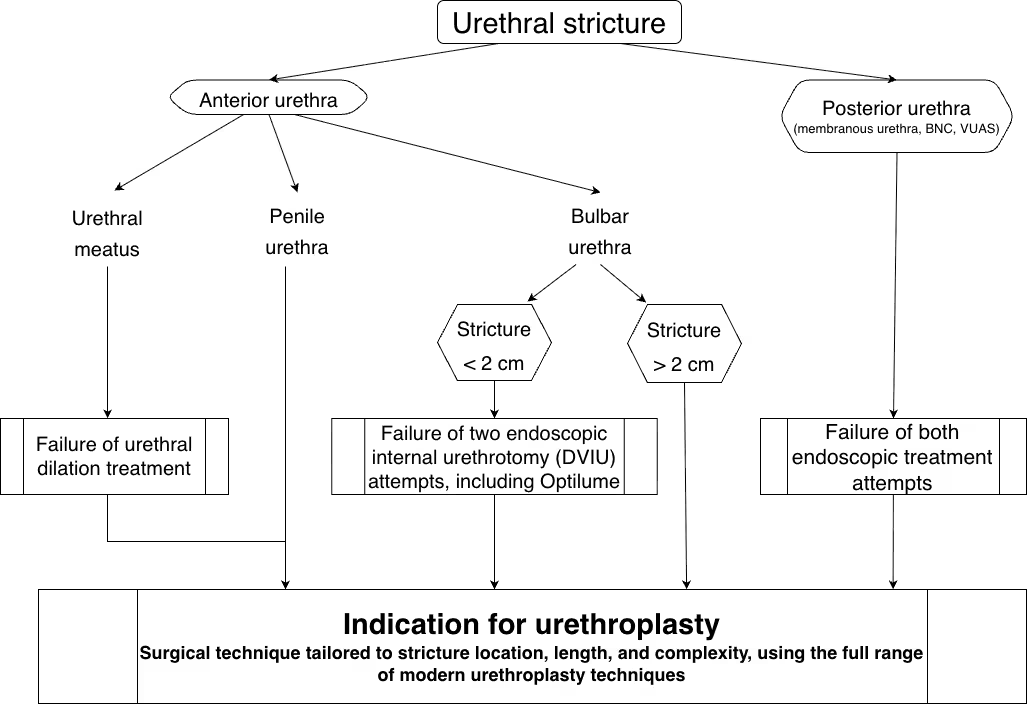
Urethral Stricture: Management Algorithm and Indications for Urethroplasty
When is urethroplasty needed?
Surgery is generally recommended when the stricture is symptomatic, recurrent, or unlikely to respond durably to simple endoscopic treatment.
Surgical treatment, most often urethroplasty, is considered when:
- Urinary symptoms are significant or progressively worsening
- The stricture recurs after endoscopic treatments (dilation or internal urethrotomy)
- The narrowing is long, dense, or complex
- There is complete obstruction
- Complications occur (recurrent infections, bladder dysfunction, urinary retention)
- The patient wishes a definitive and long-term solution
In short, surgery is indicated when the goal is durable cure rather than temporary relief. Urethroplasty offers the highest long-term success rates, particularly for recurrent or complex strictures.
Outcomes and complications of urethroplasty
Urethroplasty is currently the most effective and durable treatment for urethral stricture disease. No single technique has shown clear superiority, as each is adapted to a specific clinical situation. Overall, long-term success rates are around 80%, and may reach up to 90% in selected cases.
This is a technically demanding open surgery performed by experienced surgeons, with an overall low complication rate. The main risk remains recurrence of the stricture, occurring in approximately 10 to 20% of cases and sometimes requiring additional treatment.
Other complications are generally uncommon and often temporary. The most frequent include urinary tract infection, local swelling or bruising, and post-void dribbling. When a buccal graft is used, patients may experience temporary oral discomfort or numbness.
Less frequently, patients may develop wound infection, transient erectile dysfunction, or changes in ejaculation, which usually improve over time. More rare complications include urethral fistula or persistent sensory changes.
Overall, despite these potential risks, urethroplasty remains the reference treatment, offering the highest chance of long-term cure.
Endoscopic results after buccal mucosal graft urethroplasty for bulbar urethral stricture
Types of urethroplasty
There are several types of urethroplasty, and the choice of technique depends on the location, length, and severity of the urethral stricture, as well as patient-specific factors. The main approaches include excision and primary anastomosis (EPA), non-transecting urethroplasty, augmentation urethroplasty (typically using a buccal mucosal graft), augmented anastomotic urethroplasty, staged (two-stage) urethroplasty, and perineal urethrostomy.
Even with a thorough preoperative evaluation, the final decision regarding the most appropriate technique may only be made intraoperatively, based on direct assessment of the urethral tissue and the extent of fibrosis.
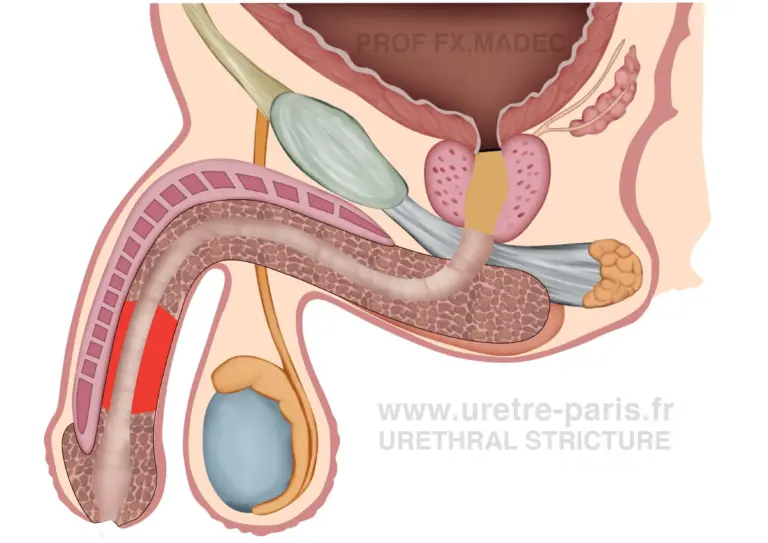
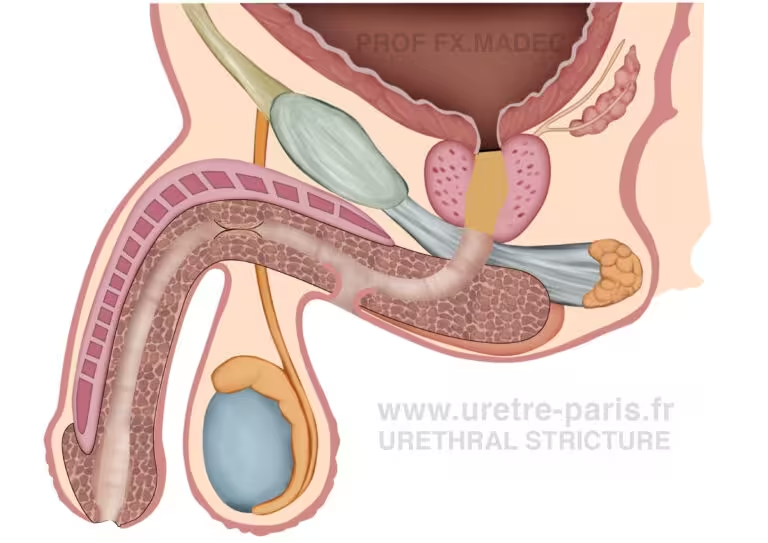
This technique consists of removing the narrowed segment of the urethra and reconnecting the two healthy ends. In some cases, a non-transecting approach can be used, which consists of removing only the diseased mucosa while preserving the other layers of the urethra.
Endoscopic results after excision and primary anastomosis urethroplasty for bulbar urethral stricture
When the stricture cannot be removed, the urethra is enlarged using additional tissue. This is most often done with a graft, typically a buccal mucosa graft (from the inside of the cheek), or with a flap using local skin tissue. The urethra is enlarged using additional tissue, either a graft or a flap. The tissue can be placed in different positions—dorsal, ventral, or both dorsal and ventral (Asopa approach). It may also be positioned either on the outside of the urethra (onlay) or inside the urinary channel (inlay). In some cases, these techniques are combined to treat longer or more complex strictures.
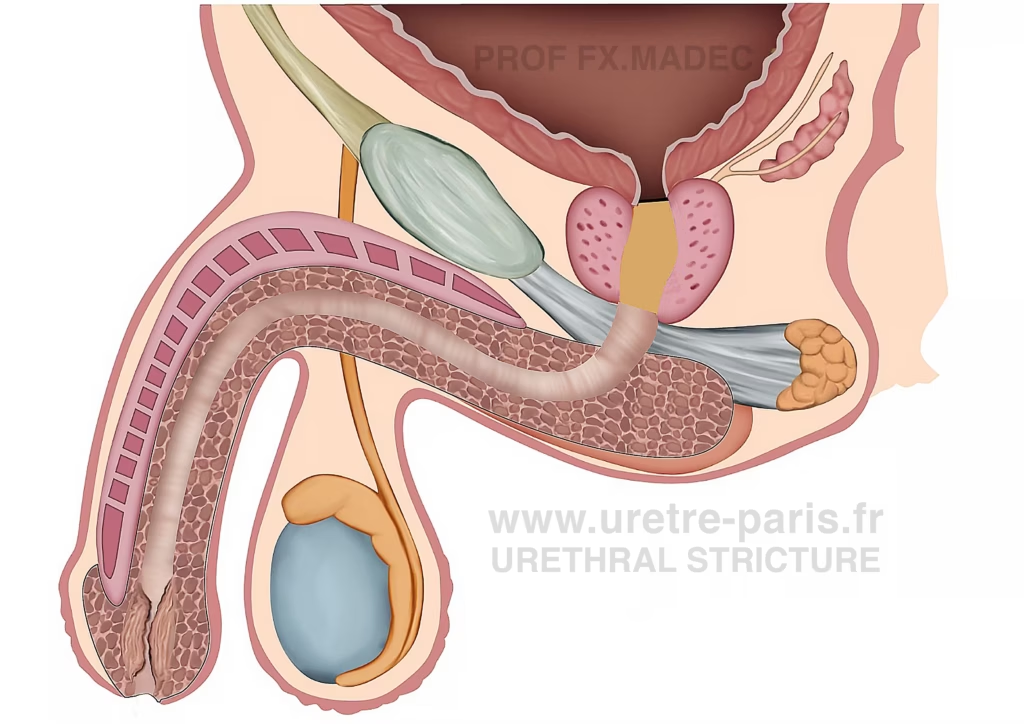
Penile urethral stricture disease requiring reconstructive urethroplasty
Dorsal onlay buccal mucosal graft urethroplasty for urethral stricture
Bulbar urethral stricture treated with ventral onlay buccal mucosal graft urethroplasty
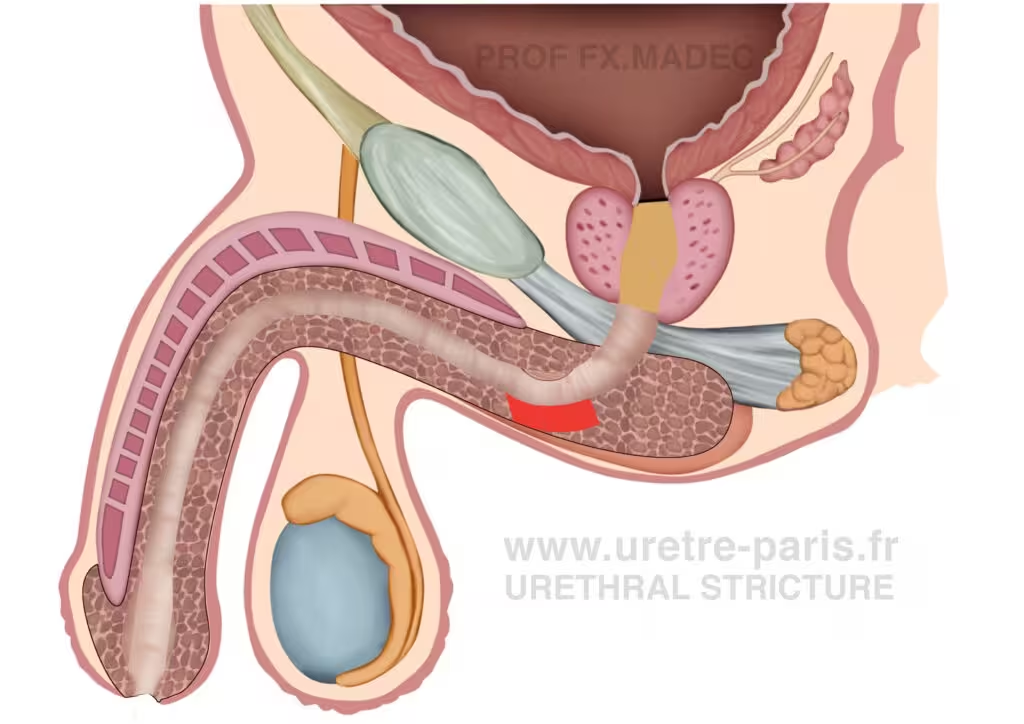
Distal urethral stricture disease involving the meatus (meatal stenosis), fossa navicularis, and penile urethra
Distal urethral stricture repair with glans-preserving meatoplasty and dorsal buccal mucosal graft urethroplasty
In some complex strictures, both techniques are combined (Excision and primary anastomosis (EPA) and Augmentation urethroplasty). Part of the narrowed segment is removed and reconnected, while the remaining diseased area is enlarged using a graft or a flap.
Complex bulbar urethral stricture before non-transecting augmented anastomotic urethroplasty with a dorsal buccal mucosal graft
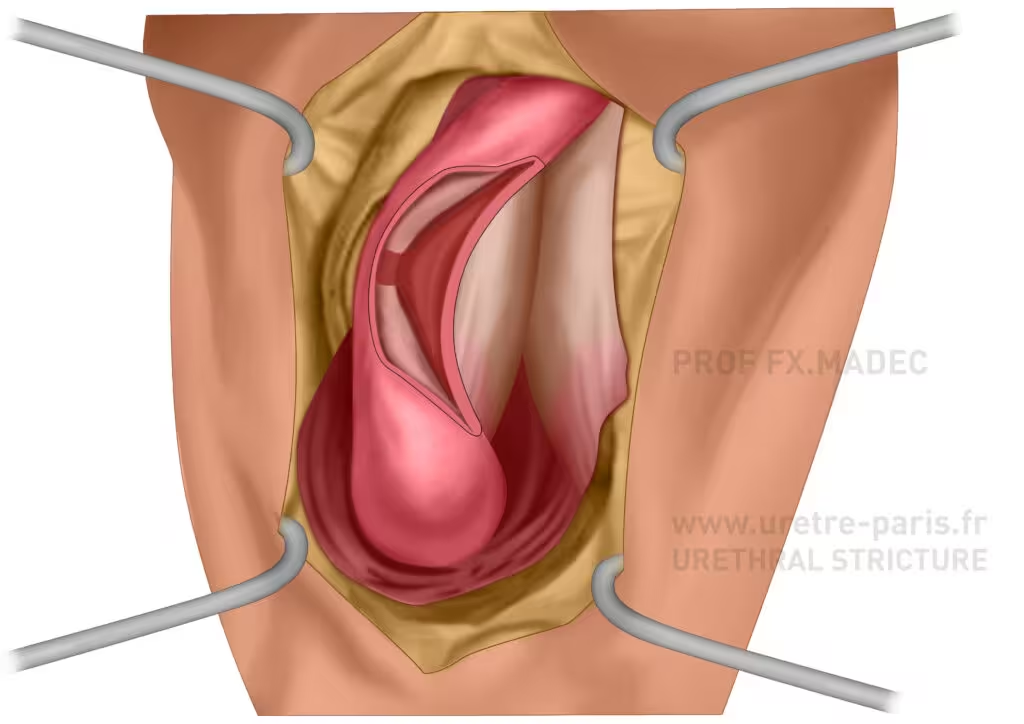
Complex bulbar urethral stricture after non-transecting stricture excision and before augmented anastomotic repair with a dorsal buccal mucosal graft
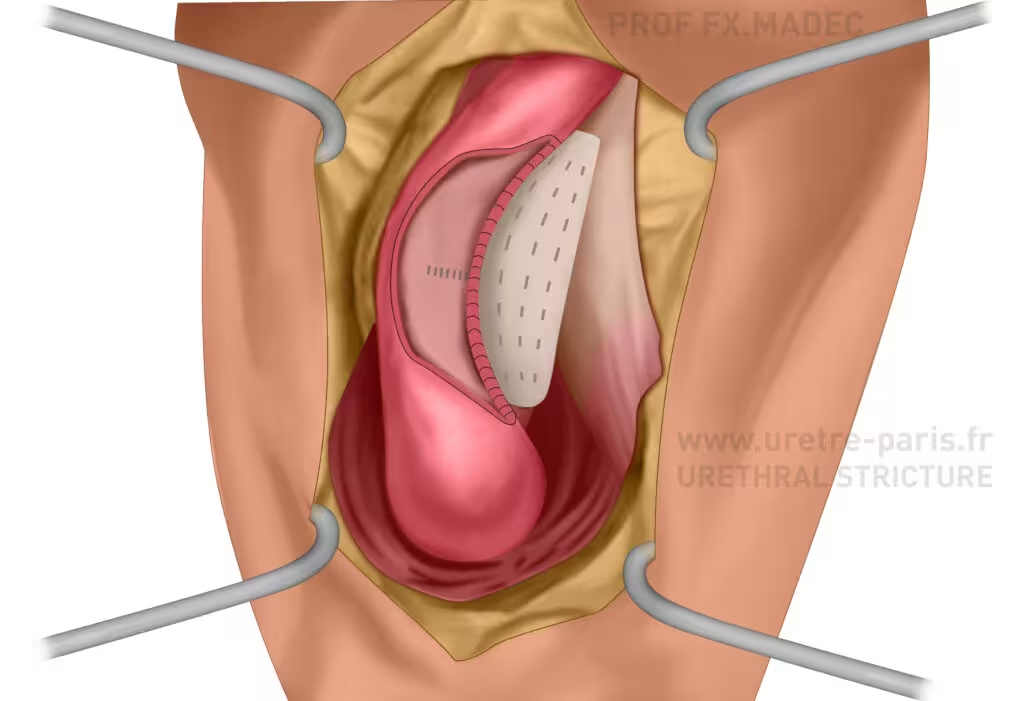
Complex bulbar urethral stricture following non-transecting augmented anastomotic urethroplasty with a dorsal buccal mucosal graft
In the most severe cases, reconstruction is performed in two stages.
The first stage consists of opening the urethra and removing the diseased segment, which is then replaced with healthy tissue laid flat. During this phase, the urinary channel is temporarily interrupted and diverted through a urethrostomy.
Several months later, a second procedure is performed to tubularize this tissue and recreate a new urinary channel.
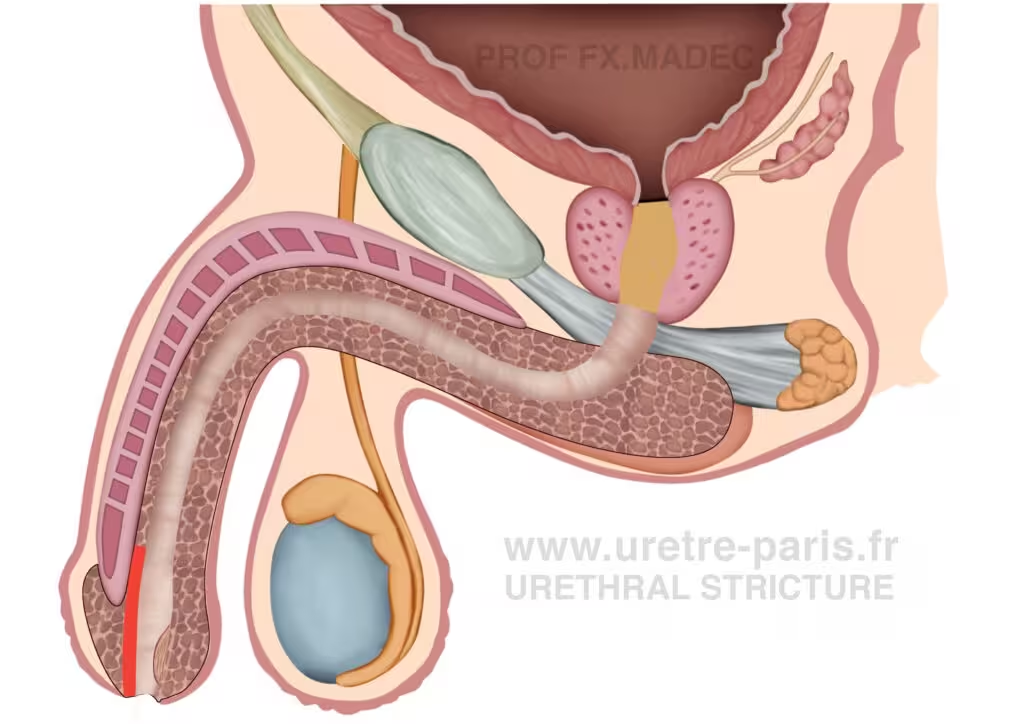
Long Penile Urethral Stricture – Frequently Encountered in Failed Hypospadias
The first stage involves opening the urethra, excising the scarred and diseased segment, and replacing it with healthy buccal mucosa graft laid flat. At this stage, the urethra is not yet tubularized, and urinary flow is temporarily diverted through a urethrostomy.
Final result after two-stage buccal mucosa graft urethroplasty for complex penile urethral stricture, showing a newly reconstructed urethral channel of adequate caliber.
In selected situations, a new opening of the urethra is created on the skin, usually in the perineal area, to allow urine to pass. This is generally proposed when reconstruction is not possible or not desired.
Perineal urethrostomy for recurrent or complex urethral stricture
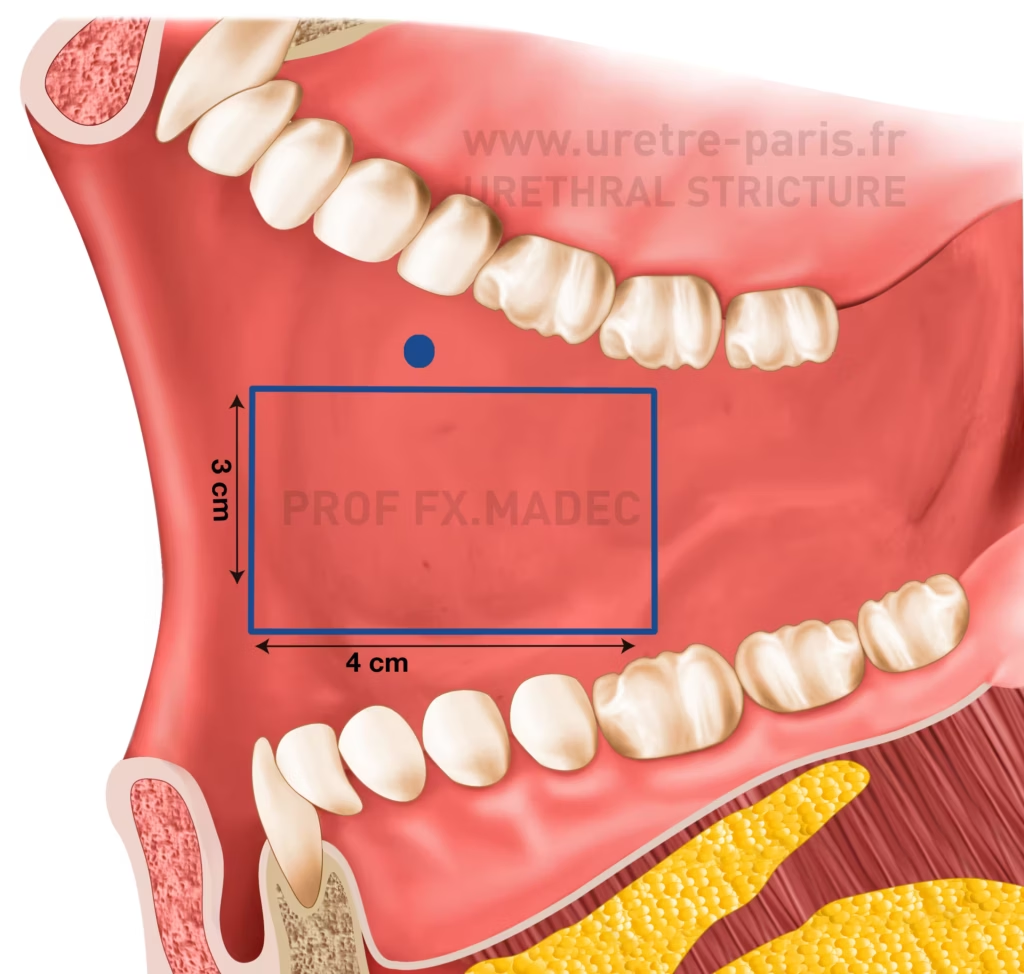
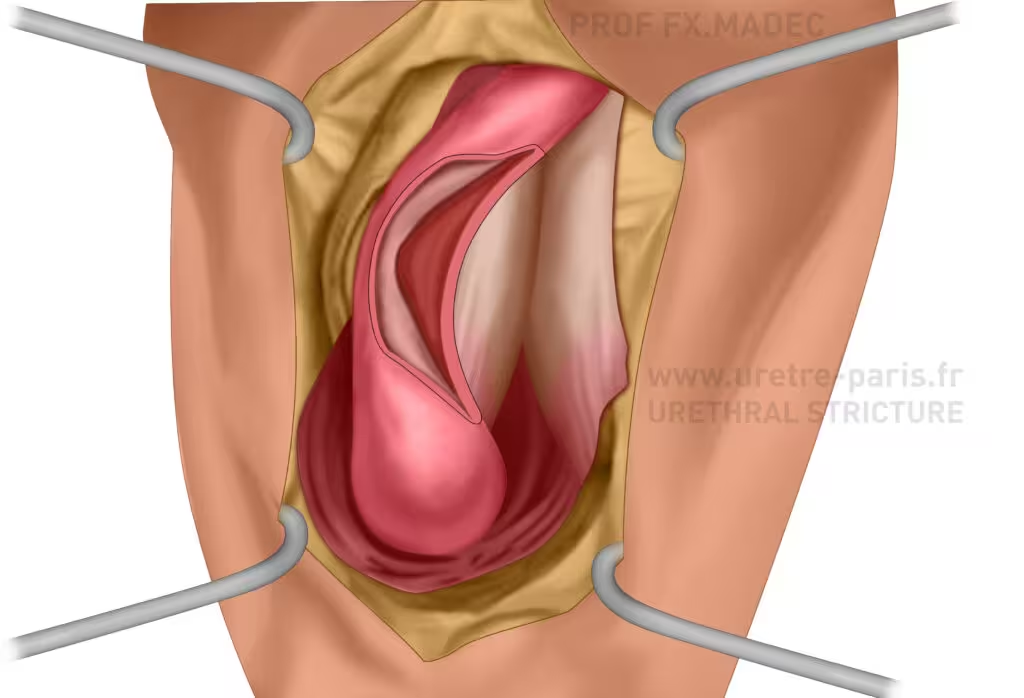
Urethral stricture repair with buccal mucosal graft (cheek graft harvest)
Buccal mucosa: the tissue of choice in urethroplasty
Buccal mucosa, especially from the inner cheek, has become the tissue of choice in urethroplasty. It is naturally adapted to a moist environment, thick, resistant to infection, and has a low tendency to shrink, which explains its high success rate.
The graft is usually 2 to 3 cm wide, and its length depends on the length of the stricture, with a minimum of about 2 cm. Complications at the donor site are uncommon and generally limited.
Why is reconstructive surgery (urethroplasty) better than simpler endoscopic treatments?
Endoscopic treatments such as internal urethrotomy or urethral dilation may temporarily improve urinary flow by cutting or stretching scar tissue, but they do not remove the underlying fibrosis. Recurrence is therefore frequent, especially in longer or recurrent strictures.
Urethroplasty, by contrast, removes or reconstructs the scarred segment using healthy tissue, often a graft. Its goal is to restore normal anatomy and provide a durable, often definitive, solution.
In patients performing self-dilatation who are considering reconstruction, urethral rest is essential. Accurate evaluation requires stopping endo-urethral manipulation so the true length and severity of the stricture can be assessed. Self-dilatation and indwelling catheters should be discontinued before imaging and surgical planning. This rest period usually lasts 12 to 16 weeks. In patients with severe symptoms or urinary retention, temporary suprapubic diversion may be required.

URETRE PARIS – Expert Center for Urethral Stricture Treatment and Urethroplasty
UNDERSTANDING URETHROPLASTY TECHNIQUES AT URETRE PARIS
At URETRE PARIS, we offer the full spectrum of modern urethral stricture treatment and urethroplasty techniques for all types of urethral stricture, including excision and primary anastomosis, non-transecting anastomotic repair, ventral and dorsal onlay augmentation urethroplasty, buccal mucosal graft urethroplasty, non-transecting augmented anastomotic urethroplasty with a dorsal buccal mucosal graft, staged urethral reconstruction, and perineal urethrostomy.
The explanatory diagrams and illustrated examples above are designed to help you understand how the urinary channel can be reconstructed and why urethroplasty is the gold-standard curative treatment for urethral stricture disease.

Urethroplasty performed by Professor François-Xavier Madec

Buccal graft harvesting for urethroplasty – Professor François-Xavier Madec

Final suturing of buccal graft urethroplasty – Professor François-Xavier Madec