Endoscopic Treatment Options
Endoscopic treatments are procedures performed through the natural urinary channel (urethra), without external incision, with the aim of reopening a narrowed segment of the urethra (stricture). Their principle remains somewhat uncertain: the aim is to widen a fibrotic urethral narrowing without causing further trauma or inducing additional scar formation. This is particularly relevant because urethral stricture is often iatrogenic, and any endourethral instrumentation may itself contribute to scarring.
Despite this paradox, endoscopic treatments have remained popular for two main reasons: they often produce an early illusion of success, with temporary symptom improvement, and they avoid open surgery, making them appear less invasive and easier to perform than urethroplasty. As a result, they have long been used as a first-line option and, in many cases, repeated unreasonably, even though they rarely provide a truly curative outcome.
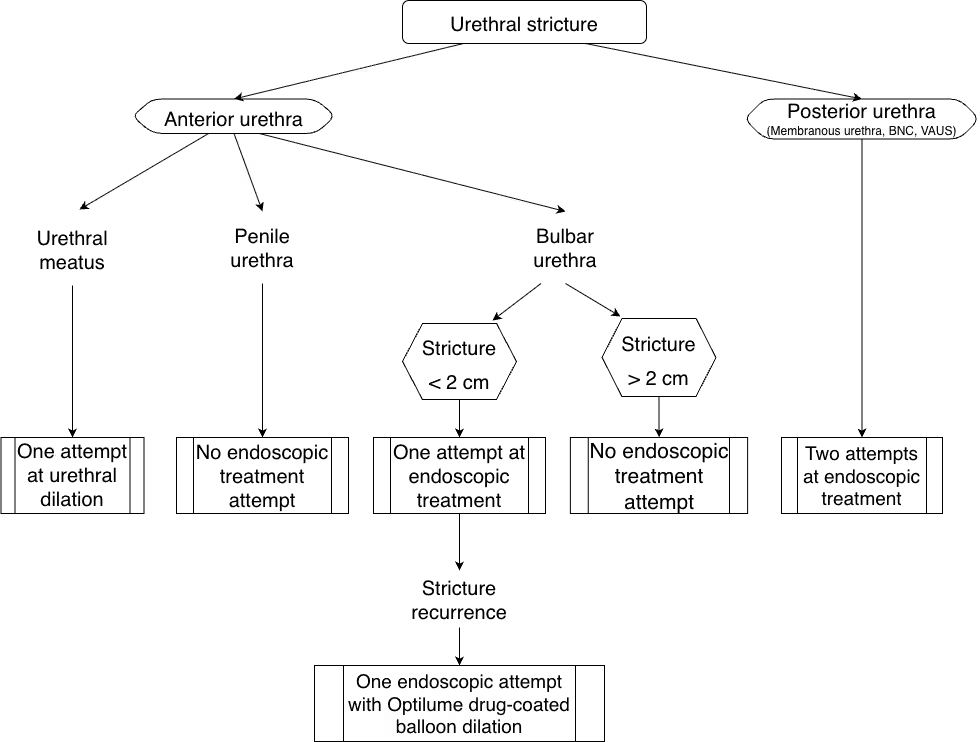
Algorithm defining the indications for endoscopic treatments and confirming their limited role in the management of urethral stricture disease.
Indications and results of endoscopic treatments in urethral stricture
Endoscopic treatments have often been overused because they are simple to perform and may create an early illusion of success, with temporary improvement in urinary symptoms during the first days or weeks.
However, urethral healing is a progressive process, and recurrence remains common over time.
For this reason, endoscopic treatment should be reserved for selected indications and limited to one or two attempts at most.
Its main indications are meatal strictures, short bulbar urethral strictures (<2 cm), and selected posterior urethral strictures.
When used in these selected situations, endoscopic treatments achieve success rates of approximately 50 to 70% after 2 to 5 years of follow-up.
By contrast, when used without appropriate selection, success rates may be much lower, ranging from around 30% down to 0%.
Their effectiveness decreases as stricture length increases, particularly beyond 2 cm, and also declines with repeated procedures.
Results are also poorer in very tight or severe strictures.
In some settings, endoscopic treatment is generally not effective, especially for penile urethral strictures.
Endoscopic techniques
There are various endoscopic techniques available for the treatment of urethral strictures. Some are innovative, while others are now largely outdated. However, their role remains limited in achieving a definitive and durable cure.
A procedure that gradually stretches the urethral stricture using bougies (thin rods) or a urinary catheter to reopen the urinary channel. It can be performed under local or general anesthesia, either in consultation or in the operating room.
An endoscopic procedure performed under direct vision that involves incising the narrowed segment of the urethra at one or more points to reopen the urinary channel. The incision can be made using different energy sources, most commonly a cold knife or a laser. It is usually performed in the operating room under short general anesthesia, and a urinary catheter is typically left in place for less than three days.
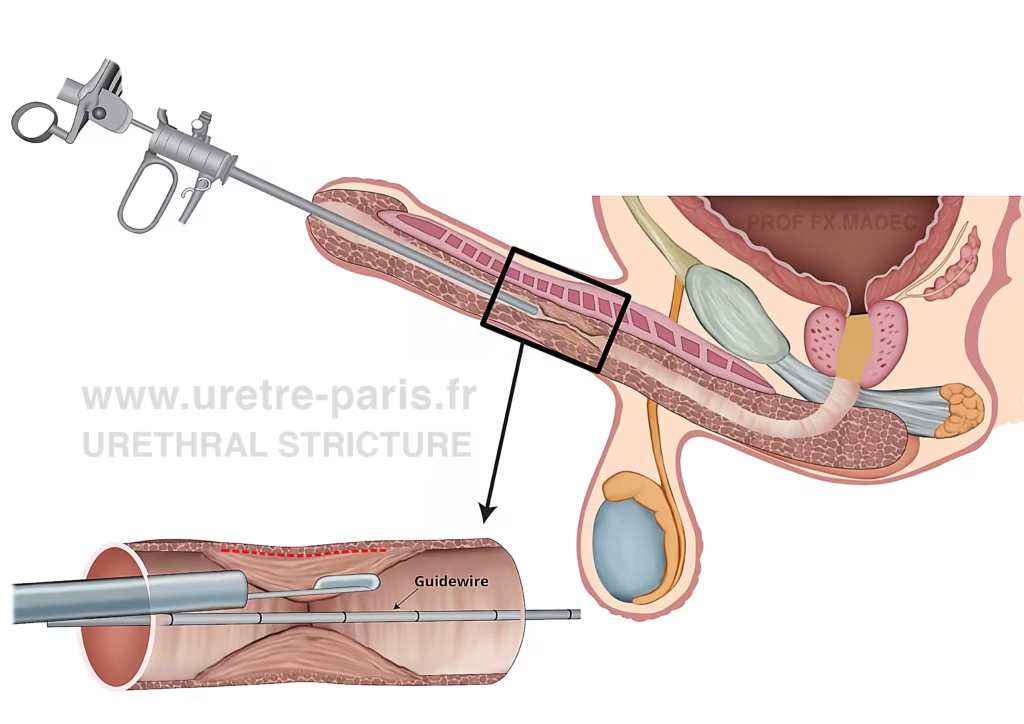
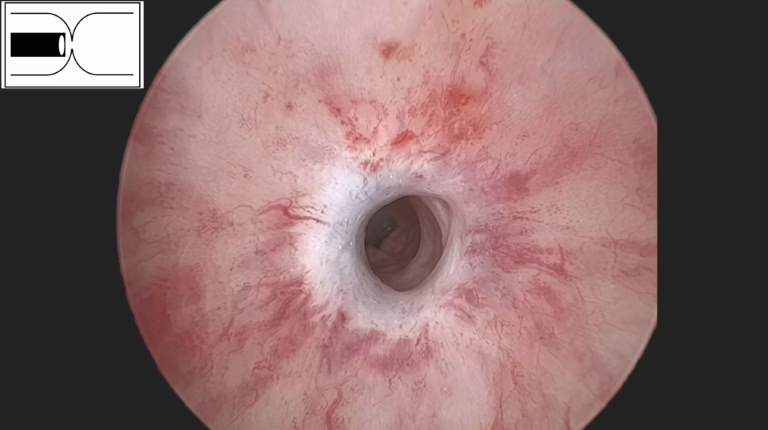
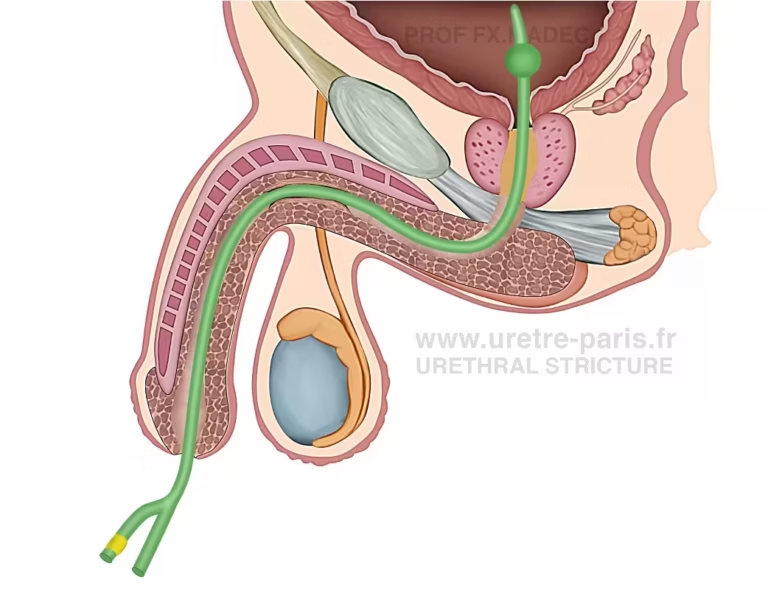
DVIU (Direct Vision Internal Urethrotomy): endoscopic treatment performed through the urethra, with placement of a fine guidewire, followed by cold-knife incision of the stenotic segment until healthy urethral tissue is reached (red dotted line).
A recent endoscopic treatment that combines a Direct Vision Internal Urethrotomy (DVIU) with the local delivery of paclitaxel (Optilume), an antiproliferative agent intended to reduce scar formation. The procedure is performed in the operating room under general anesthesia. It typically begins with an internal urethrotomy, followed by the positioning of a drug-coated balloon at the stricture site to deliver paclitaxel directly to the treated area. This technology was evaluated in the ROBUST trial and is mainly indicated for recurrent short bulbar urethral strictures (<3 cm). In this setting, reported success rates reach up to 70% at 3 years of follow-up. However, its efficacy has not been demonstrated in other situations, particularly in patients with multiple previous endoscopic treatments, or in strictures involving the meatus, penile urethra, or posterior urethra. Professor François-Xavier Madec was among the first surgeons to introduce and evaluate Optilume in France, starting in 2023. Since 2026, this treatment has been reimbursed by the national healthcare system.
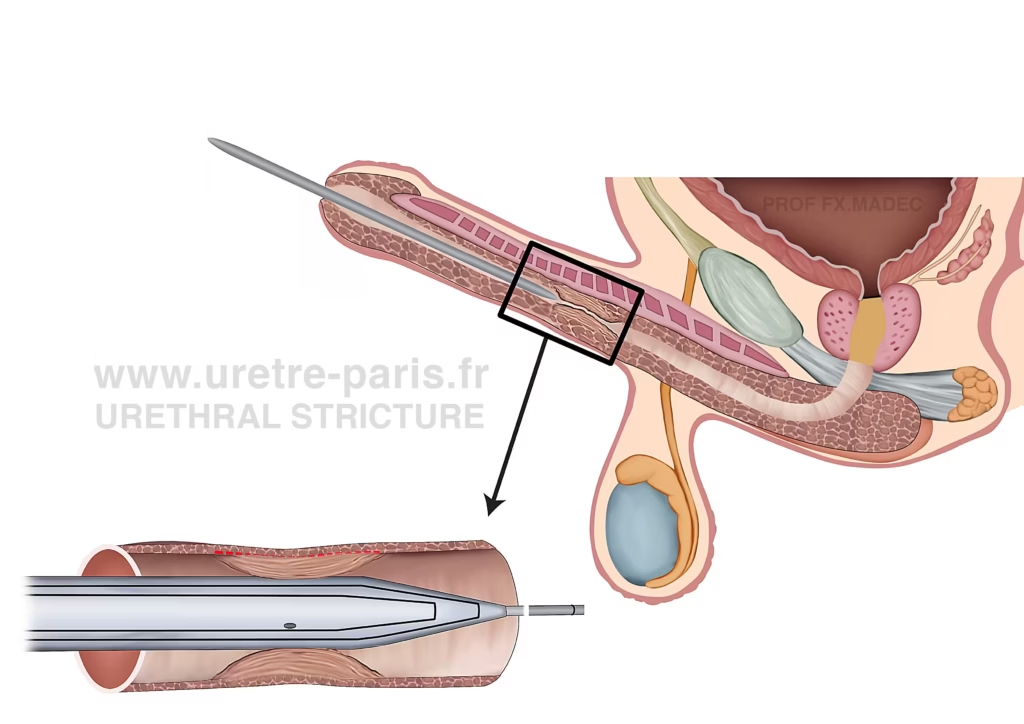
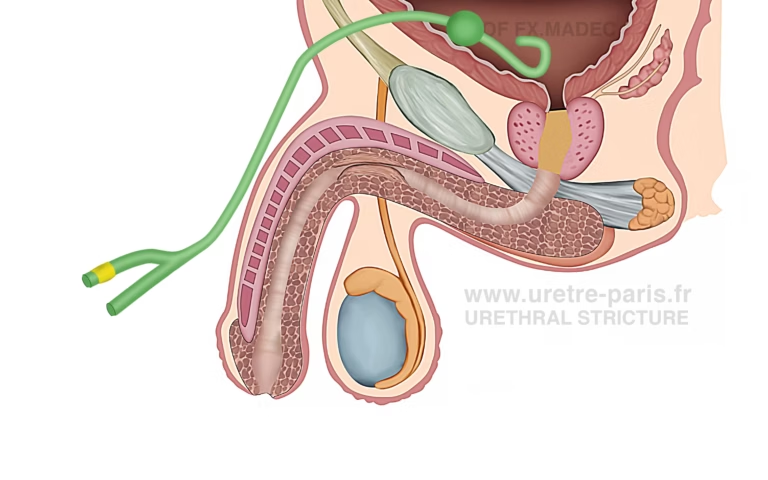
Optilume procedure: after DVIU (Direct Vision Internal Urethrotomy), defined as a cold-knife endoscopic incision of the urethral stricture, the paclitaxel-coated Optilume balloon is positioned across the treated segment.
Endoscopic Treatment Journey
DVIU and drug-coated balloon dilation (Optilume) are generally performed as short procedures, either as day surgery or with one overnight hospital stay. The urinary catheter is usually removed at home, typically within the first 3 postoperative days. Recovery is usually rapid. Sick leave is generally limited to a few days. Sports can usually be resumed after 2 weeks, and sexual activity after about 1 month.
A technique in which the patient performs urethral dilatation at regular or intermittent intervals using a catheter to keep the urinary channel open. It is generally not recommended for most urethral strictures. Its role is mainly limited to patients who are not suitable for surgery, those with multiple reconstructive failures, or selected cases of complex prostato-membranous strictures, particularly after radiotherapy. When proposed, it should be regarded as a palliative rather than curative option, as it maintains urethral patency without resolving the underlying scar disease. Patients should be informed of its impact on quality of life, as well as the risk of repeated discomfort and complications. Repeated urethral trauma may also worsen and further complicate the stricture over time. If reconstructive surgery is reconsidered later, accurate reassessment of the stricture may be challenging. A period of urethral rest, with no urethral instrumentation for several weeks, is often required to allow complete healing and reliable imaging evaluation. During this interval, the risk of urinary retention must be anticipated.
A technique that involves placing a small metallic device (stent) inside the urethra to keep the narrowed segment open. This approach was previously used as an alternative to repeated endoscopic treatments. However, it has been largely abandoned due to a high rate of complications (pain, migration, tissue overgrowth). Many patients ultimately required surgical removal of the stent, often followed by urethroplasty. Today, covered metallic stents may still be considered as a temporary option in highly selected patients who are not candidates for reconstructive surgery.
In rare situations, the urethral condition is so complex that long-term urinary drainage must be considered. This may involve either a transurethral catheter (after endoscopic treatment) or a suprapubic catheter, usually placed under local anesthesia. Such management should remain exceptional, as chronic catheterization is associated with recurrent urinary tract infections, urethral damage, and progressive impairment of bladder and kidney function. It should therefore be avoided whenever possible, except in patients with very limited life expectancy or no reasonable reconstructive option.
Urethral stricture poorly managed with long-term indwelling urinary catheter
Urethral stricture temporarily managed with suprapubic catheter before urethroplasty
Conclusion
At URETRE PARIS, we offer the full spectrum of modern endoscopic treatments for urethral stricture, including Optilume, with careful respect for proper indications. These techniques are used thoughtfully and without overuse, as endoscopic management is not appropriate in every case. In case of failure, or when a durable reconstructive approach is more suitable, we do not hesitate to recommend urethroplasty.