- Home
- Understanding Urethral Stricture
Understanding Urethral Stricture
This page provides a complete overview of urethral stricture disease, including what it is, why it occurs, how it is diagnosed, and the available treatment strategies from endoscopic management to definitive urethroplasty.
It is designed to help patients understand their condition and make informed decisions about specialist reconstructive care.

Urethral Anatomy and Function
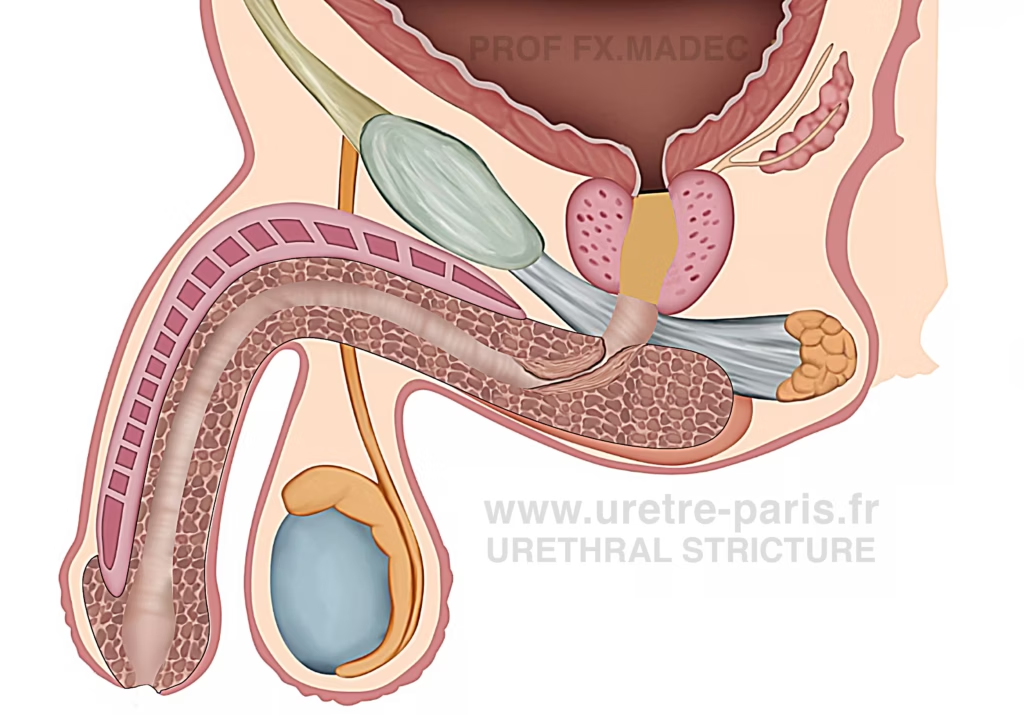
The urethra is a musculo-membranous tube that carries urine from the bladder to the outside of the body. In men, it also carries semen.
The male urethra measures about 20 cm and is divided into two main segments:
- the anterior urethra, including the bulbar urethra, penile urethra, and urethral meatus
- the posterior urethra, including the prostatic urethra, membranous urethra, and bladder neck, with the sphincter mechanisms
The urethra has a segmental blood supply: the posterior urethra is mainly supplied by pelvic arteries, whereas the anterior urethra receives blood from branches of the internal pudendal artery. Venous drainage follows similar pathways through the periprostatic plexus and internal pudendal venous system.
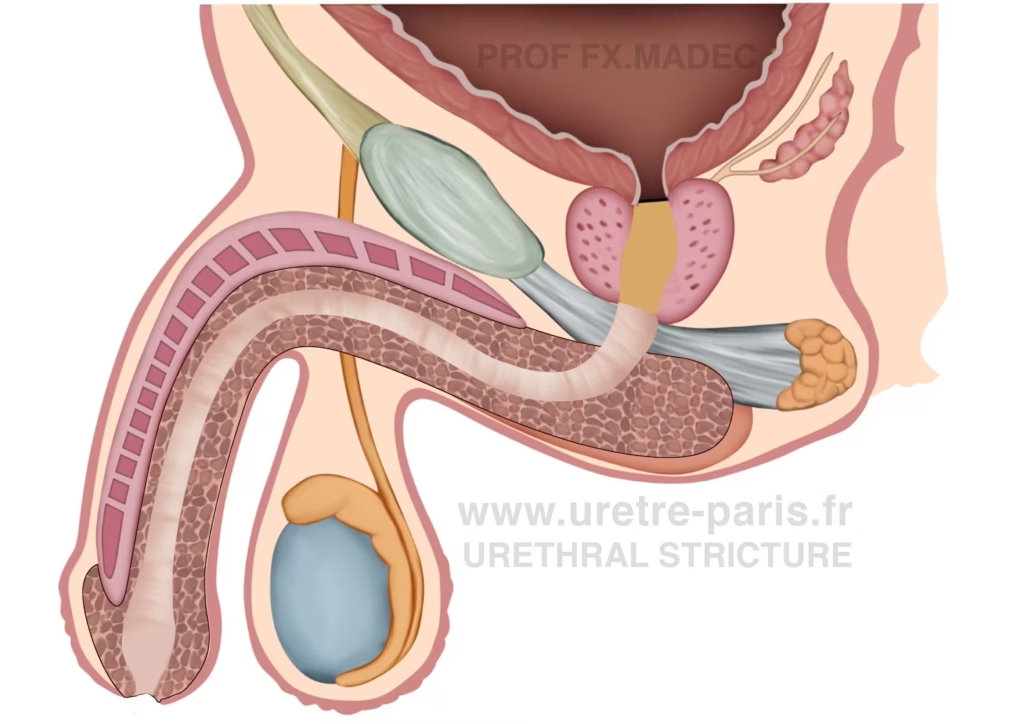
Normal urethra: uniform caliber of the urinary channel without any narrowing.
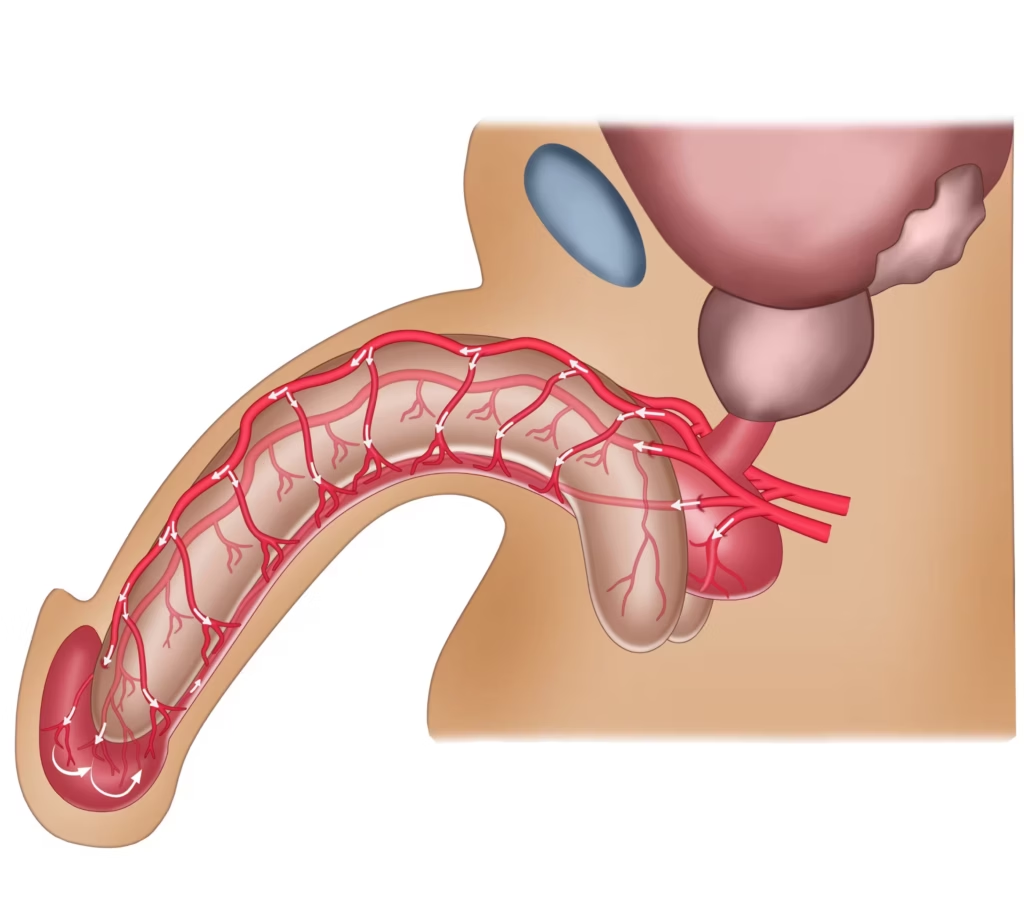
Dual arterial blood supply of the urethra
The urethra receives blood from two directions, which helps maintain tissue health. One part comes from arteries supplying the urethra directly, and another comes from the glans and surrounding tissues.
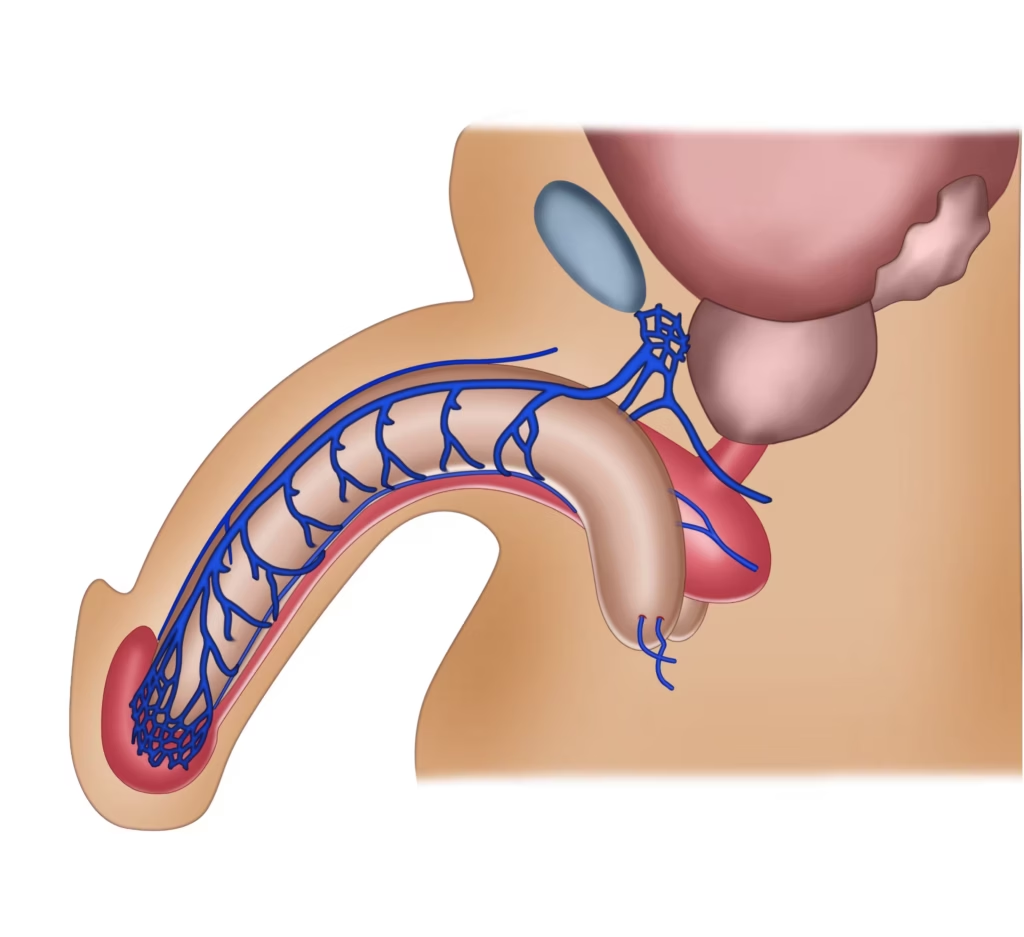
Venous Vascularization of the urethra. The venous drainage of the urethra follows the penile veins and drains mainly into the periprostatic (Santorini’s) venous plexus.
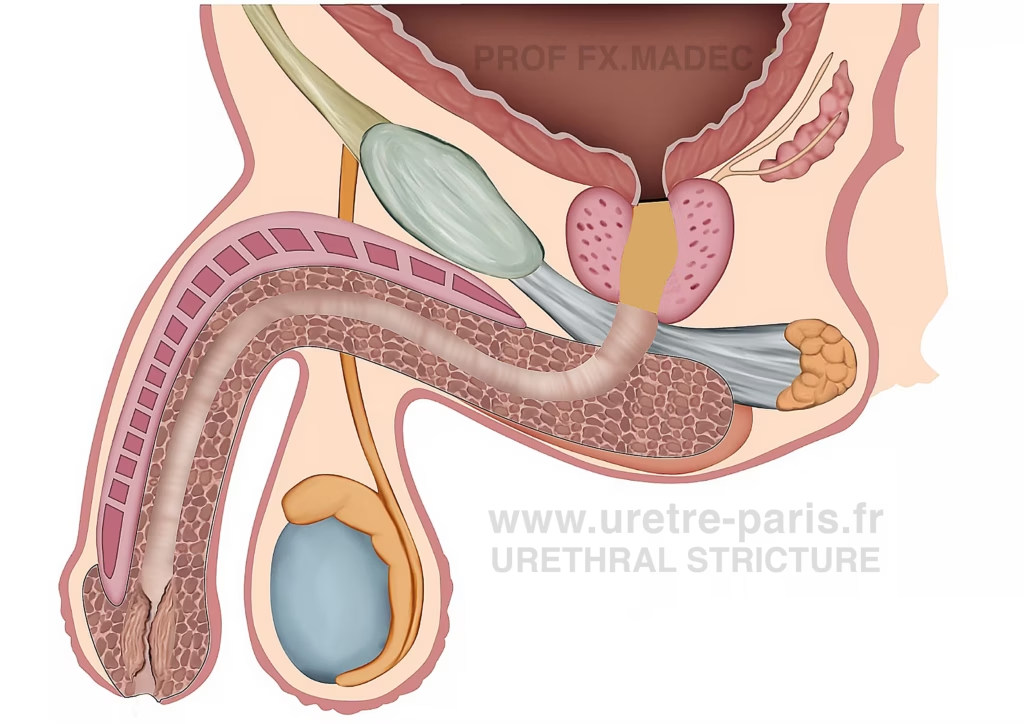
What is a urethral stricture in simple terms?
In simple terms, a urethral stricture is a narrowing of the urethra caused by scar tissue.
The urethra is the tube that carries urine from the bladder to the outside of the body. When scar tissue forms inside this tube, it reduces its diameter, making it harder for urine to pass.
This narrowing can slow the urinary stream, cause difficulty emptying the bladder, and in severe cases lead to urinary retention.
Meatal stenosis
Narrowing of the urinary channel located at the tip of the penis, in the region of the urethral meatus (glans).
Bulbar urethral stricture
The most common location of urethral strictures, involving a narrowing in the proximal (bulbar) segment of the urethra.
What causes it?
Idiopathic – In many cases, no clear cause is identified despite thorough evaluation.
Iatrogenic (medical procedures) – is the most common identifiable cause. This includes urethral catheterization, cystoscopy, prostate surgery (for benign prostatic enlargement), radical prostatectomy, radiotherapy, or prior urethral surgery, failed hypospadias repair (post-hypospadias strictures).
Trauma – direct perineal injuries (e.g., straddle injuries) can damage the urethra and lead to scarring as well as Pelvic fractures.
Inflammatory conditions – Particularly lichen sclerosus (balanitis xerotica obliterans), which can cause progressive fibrosis.
Infections – Historically common (especially gonorrhea), now less frequent in industrialized countries.
How common is it?
Urethral stricture affects approximately 1 in 100 men, with prevalence increasing after the age of 50. The anterior urethra is most commonly involved, particularly the bulbar segment. In France, more than 20,000 procedures are performed each year for this condition. However, fewer than 5% are true reconstructive surgeries (urethroplasties), although this approach is considered the most effective and definitive treatment in many cases.
What symptoms should make someone worry?
This narrowing of the urinary channel leads to obstruction of urine flow, resulting in symptoms such as a weak stream, straining, prolonged urination, incomplete emptying, or recurrent infections. Some men may also experience ejaculatory symptoms, including pain or reduced force.
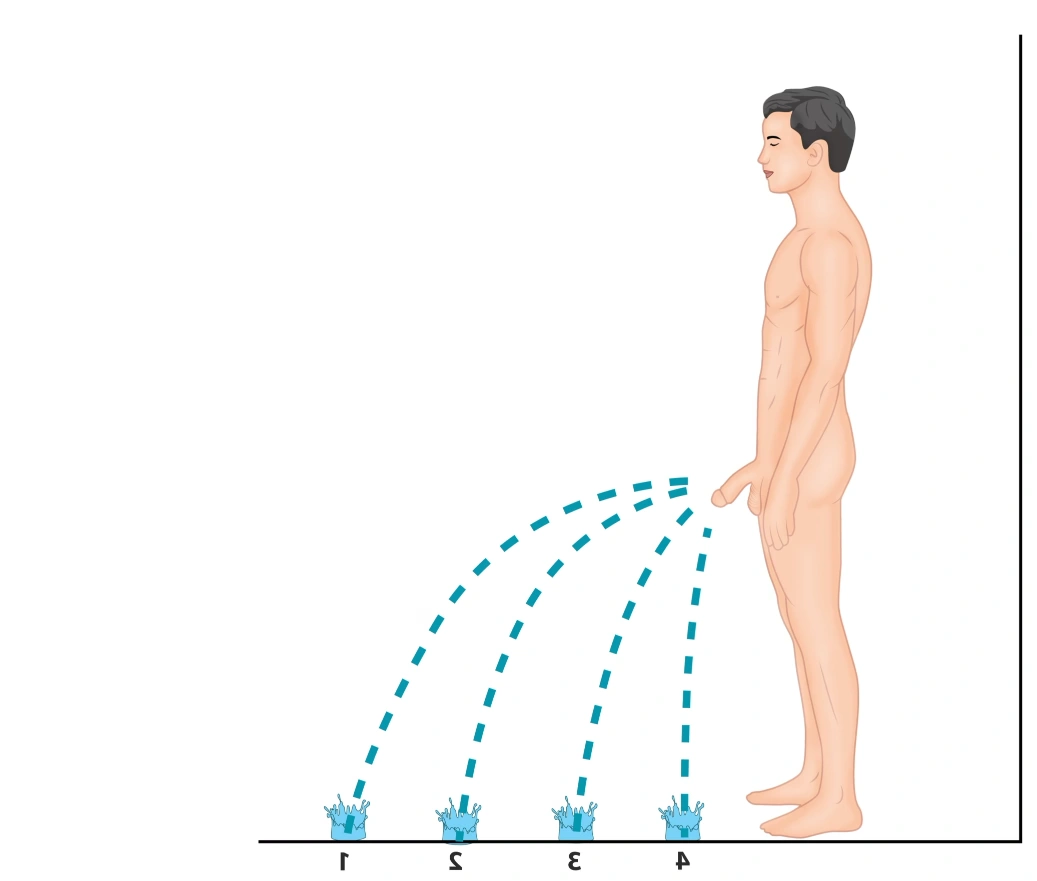
Decrease in urinary flow (1–4) according to urethral stricture severity.
When should they consult a specialist?
Patients should seek urological evaluation if they notice a persistent or worsening reduction in urinary flow, with a stream that becomes weaker, slower, or more difficult to pass.
Diagnosis
How is it diagnosed?
Urethral stricture is diagnosed through a combination of symptoms, physical examination, and imaging or endoscopic evaluation.
What tests are typically used?
The diagnostic work-up typically includes:
Clinical history – Symptoms, prior procedures, trauma, or infections may suggest a stricture.
Uroflowmetry + Post-void residual – Measures urinary flow and bladder emptying.
Flexible cystoscopy (endoscopy of the urethra) – A small camera is used to look inside the urethra.
Urethral imaging – Defines location, length, and severity of the stricture:
- Urethral X-ray (RUG/VCUG) – Contrast is injected into the urethra to visualize the narrowing
- CT scan of the urethra (CT urethrography) – Advanced imaging in selected or complex cases
- MRI of the urethra (MR urethrography) – High-resolution imaging for detailed assessment
In summary, diagnosis is confirmed by imaging and/or endoscopic visualization, which allow precise characterization of the stricture before deciding on treatment.
Treatment Overview
Treatment depends on the stricture’s location, length, severity, and prior treatments.
Urethroplasty (reconstructive surgery)
This is definitive surgical repair of the urethra. Different techniques are used depending on the case (excision and primary anastomosis, grafts such as buccal mucosa, or flap reconstruction). Urethroplasty offers the highest long-term success rates and is typically performed in specialized centers.
Active surveillance (“watchful waiting”)
In selected mild cases with limited symptoms, simple monitoring may be appropriate.
The goal of treatment is to restore a durable opening of the urinary channel
Internal urethrotomy (optical urethrotomy)
An endoscopic procedure performed through the natural urinary channel. The scar tissue is incised internally to widen the urethra. It is minimally invasive but recurrence is common, especially for longer or recurrent strictures.
Urethral dilations
Progressive widening of the urethra using plastic or metal dilators. In some cases, intermittent self-dilation may be required. This approach can relieve symptoms but does not remove the scar tissue.
Drug-coated balloon dilation (Optilume®)
A balloon dilation combined with local drug delivery. It may be proposed in selected cases, particularly for short (< 3 cm) recurrent bulbar strictures.
Urethral stoma (urethrostomy)
In complex cases, the diseased segment may be bypassed and the healthy urethra brought directly to the skin. Depending on location, this may be a meatostomy or a perineal urethrostomy.
Long-term urinary drainage
In patients unfit for surgery or in selected situations, long-term catheterization (urethral catheter or suprapubic catheter) may be necessary.
Why should patients seek a specialist for this condition?
Urethral stricture is a complex condition that requires precise evaluation and individualized management.
A specialist in reconstructive urology can:
- Accurately assess the location, length, and severity of the stricture
- Differentiate between simple and complex cases
- Avoid repeated ineffective treatments that may worsen scar tissue
- Offer the full range of therapeutic options, including definitive reconstructive surgery
- Optimize long-term outcomes and reduce recurrence risk
Repeated dilations or urethrotomies without proper assessment can increase fibrosis and make future reconstruction more challenging.
In short, early evaluation by a specialist helps ensure the right treatment strategy from the beginning, improving both success rates and quality of life.
What is Professor Madec’s specific experience with this disease?
Urethral stricture disease, and especially urethral reconstruction (urethroplasty), is a highly specialized field within urology that requires specific training and extensive experience.
Professor François-Xavier Madec is recognized as a national referral expert in this area and regularly receives patients referred by urologists across France for expert evaluation and management of complex strictures. These include recurrent strictures after endoscopic treatment, any type of urethral stricture requiring urethroplasty, long or multi-segment strictures, post-hypospadias strictures, post–prostate cancer strictures (including post-radiation strictures and vesicourethral anastomotic stenosis), and cases with multiple prior failed procedures.
Management is based on an individualized reconstructive approach aimed at achieving durable functional outcomes.
The full spectrum of urethroplasty techniques is offered according to stricture location, length, etiology, and tissue quality. These include buccal mucosa graft urethroplasty, performed as one-stage or staged procedures, with ventral, dorsal, or combined graft placement. Excision and primary anastomosis is also performed, including transecting and non-transecting techniques, as well as meatoplasty, perineal urethrostomy, and repair of urethral fistulas using flap-based reconstruction when needed.
This expertise is supported by active participation in multidisciplinary case discussions dedicated to urethral stricture disease, including the CHARRUES meetings within the French Association of Urology, helping guide complex diagnostic and therapeutic decisions.
It is also supported by extensive surgical experience, with hundreds of urethroplasties performed, and by a strong academic commitment to reconstructive urology and genital reconstruction, with urethral stricture disease representing a major focus of published work.
What should a patient do if they think they have this problem?
If a patient notices persistent urinary symptoms—such as a weak stream, straining, prolonged voiding time, or recurrent urinary infections—the first step is to consult a general urologist.
Step 1: Initial evaluation by a urologist
A urologist will:
- Take a detailed medical history (prior catheterization, prostate treatment, trauma, surgery)
- Perform basic tests such as uroflowmetry and bladder ultrasound
- Decide whether imaging or endoscopic evaluation is necessary
This first assessment confirms whether a urethral stricture is suspected.
Step 2: Referral to a reconstructive urethral specialist (if needed)
If the stricture is confirmed, recurrent, long, complex, or related to prior surgery or radiation, referral to a specialist in urethral reconstruction is recommended.
A reconstructive expert can:
- Perform detailed imaging analysis
- Classify the stricture precisely
- Avoid repeated ineffective endoscopic treatments
- Propose definitive surgical options when appropriate
In summary, initial evaluation is essential, but complex or recurrent cases benefit from assessment by a dedicated urethral reconstructive specialist to optimize long-term outcomes.