Diagnosis & Evaluation
The diagnosis of a urethral stricture is based on several complementary steps: assessment of symptoms, medical history, clinical examination, followed by additional investigations to confirm the stricture and define its location, length, and severity.

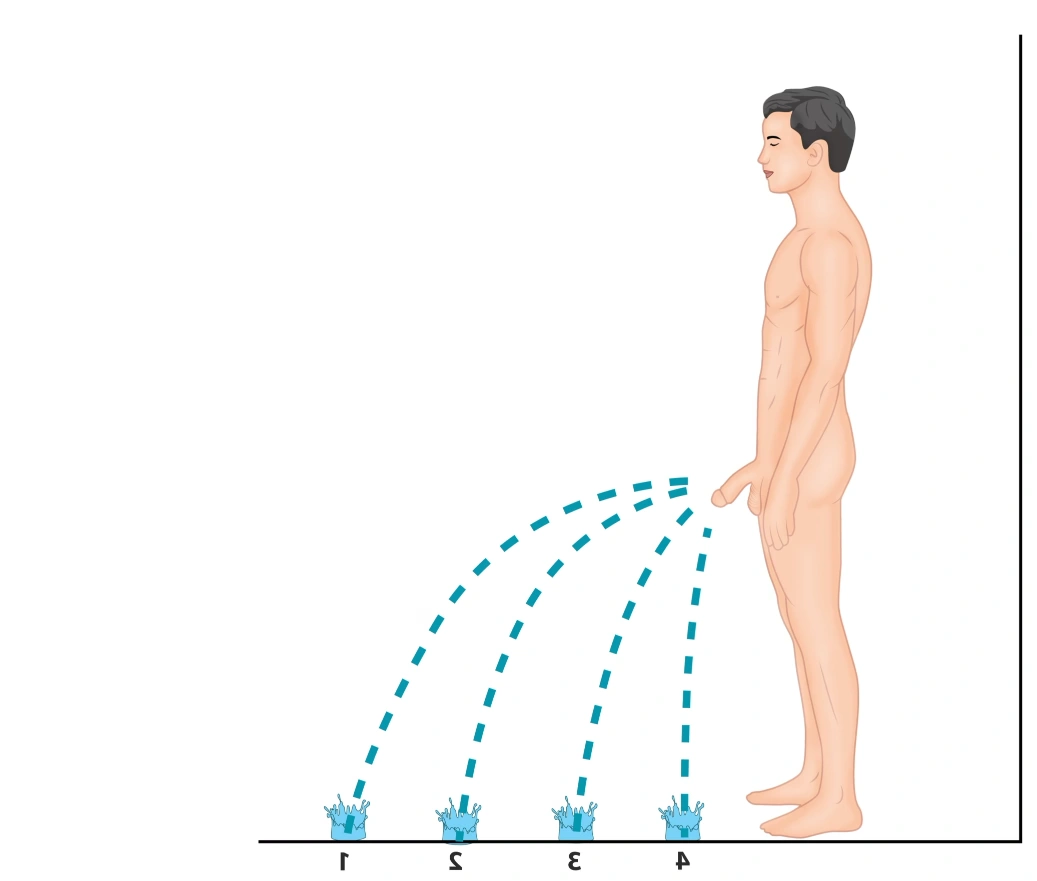
Decrease in urinary flow (1–4) according to urethral stricture severity.
What Signs Should Raise Concern?
In most cases, urethral stricture presents with urinary symptoms such as a weak stream, difficulty urinating, or a sensation of incomplete bladder emptying. Acute urinary retention may also reveal the condition. Less commonly, it is diagnosed following a urinary tract infection or difficulty during catheterization.
Symptoms may affect different phases of urination:
- During urination: weak stream, straining, pain or burning, intermittent flow
- Before urination: urgency, increased frequency, sometimes urge incontinence
- After urination: post-void dribbling due to urine pooling upstream of the stricture
Other warning signs include a split urinary stream, persistent burning, recurrent urinary tract infections, perineal pain, or ejaculatory disorders.
Finally, some strictures may remain minimally symptomatic or even silent, and are discovered incidentally during investigations performed for another reason.
During the consultation, the doctor will review your symptoms and look for possible causes of urethral stricture, such as:
- previous urinary or hypospadias surgery
- perineal trauma
- Prior medical procedures such as urethral catheterization, endoscopic examination of the urethra, or repeated urethral instrumentation
- prostate treatment
- certain sexually transmitted infections
- Lichen sclerosus (balanitis xerotica obliterans)
This discussion also helps clarify:
- when the urinary symptoms began and how they have changed
- their severity
- any previous treatments and their results
- any associated symptoms such as pain, infections, or sexual difficulties
- your overall health
Patient-Reported Outcome Questionnaires
Specific questionnaires can help more precisely assess the burden related to urethral stricture:
Evaluates urinary symptoms and their impact on quality of life
Ejaculatory Dysfunction (MSHQ-EjD)
Assesses erectile function
Specific questionnaires can help more precisely assess the burden related to urethral stricture:
Urethral stricture self-assessment questionnaires
Download the questionnaire above
The clinical examination is systematic, comprehensive, and usually non-invasive. It includes:
- examination of the penis, urethral meatus, and foreskin to identify lichen sclerosus, scarring, or a narrowed meatus
- palpation of the penis and perineum to detect fibrosis, tenderness, fistula, or diverticulum
- examination of the scrotum
- sometimes photographs of the erect penis, in case of prior surgery or penile curvature
- abdominal palpation to assess for a distended bladder or hernia
- examination of the oral cavity prior to possible buccal mucosa graft harvesting
Additional Investigations for the Diagnosis of Urethral Stricture
Once symptoms have been identified and the clinical examination completed, several investigations can be performed to confirm the presence of a urethral stricture and to assess its location, severity, and length. However, before interpreting these tests, one essential principle must be respected: urethral rest.
Urethral healing follows three phases: inflammation, proliferation, and remodeling. In the absence of repeated urethral trauma, the scar progressively stabilizes, reaching about 80% of its final strength after 6 weeks, while continuing to mature for several months. Accurate evaluation of a urethral stricture therefore requires a period without endo-urethral manipulation, in order to correctly assess its true extent, particularly its length and degree of narrowing. Indwelling catheters should be removed and intermittent self-dilatation discontinued before imaging and surgical planning. This period of urethral rest typically lasts 12 to 16 weeks. In patients with severe symptoms or urinary retention, temporary urinary diversion with a suprapubic catheter is recommended.
Uroflowmetry involves urinating into a device that measures the flow rate and volume of the urinary stream. In cases of urethral stricture, the flow is often reduced, with a typical “plateau” pattern, helping to assess severity. This test is usually complemented by a bladder ultrasound to measure the post-void residual (PVR), i.e., the amount of urine remaining in the bladder after urination. A high residual may indicate a more severe stricture and sometimes requires temporary drainage.
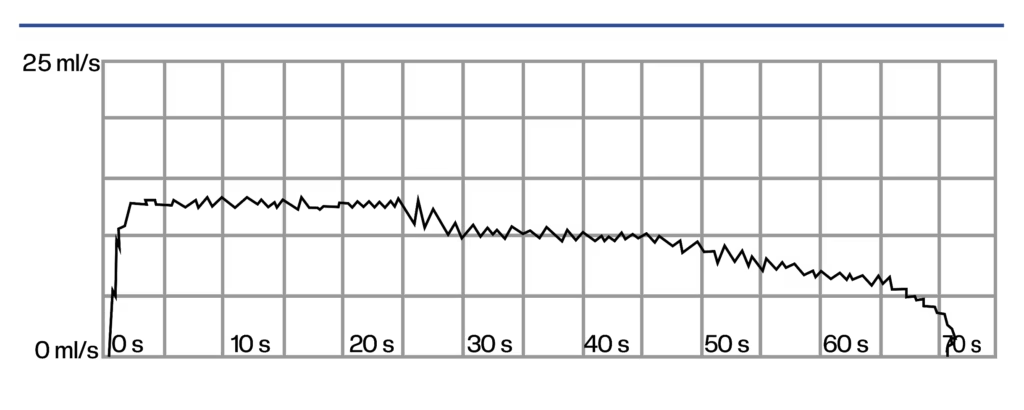
Typical uroflowmetry findings in urethral stricture: maximum flow rate below 15 mL/s, plateau-shaped curve, and prolonged voiding time exceeding 45 seconds.
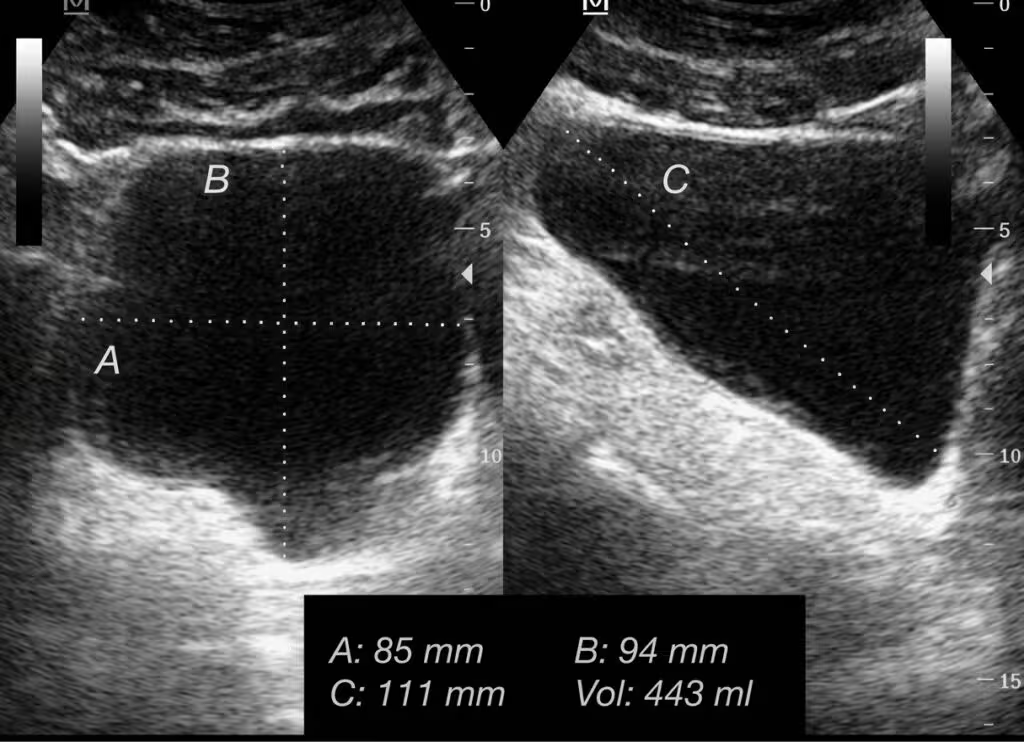
Bladder ultrasound showing a significant post-void residual: in this patient with urethral stricture, the bladder does not empty properly.
Flexible cystoscopy allows examination of the inside of the urethra using a small flexible camera. It is one of the most reliable tests for confirming a urethral stricture. If the scope cannot pass through, this confirms the presence of a narrowing. Endoscopy also helps assess the mucosa and identify lichen sclerosus, inflammation, a tumor, or a stone. It can accurately locate the distal end of the stricture. However, it does not always assess the full extent of the stricture, especially when it is long or complete. In such cases, additional investigations are required.

Endoscope inserted into the urethra under local anesthesia.
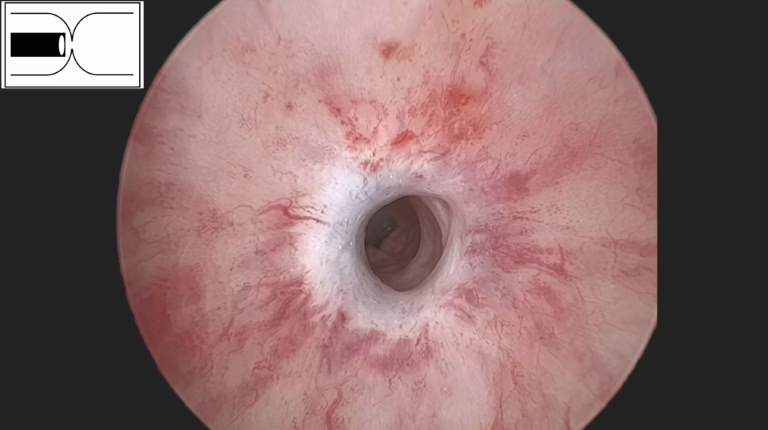
Endoscopic images of a urethral stricture, demonstrating a narrowed fibrotic ring within the urethral lumen.
Urethrocystography is a key imaging test used to clearly visualize the urethra and confirm the presence of a stricture. It provides precise information on its location, length, and severity, which are essential for choosing the appropriate treatment.
- Retrograde phase: a contrast agent is gently injected through the urethra to visualize the urethra and identify the narrowing
- Voiding phase: performed while you urinate, allowing assessment of the posterior urethra and bladder emptying
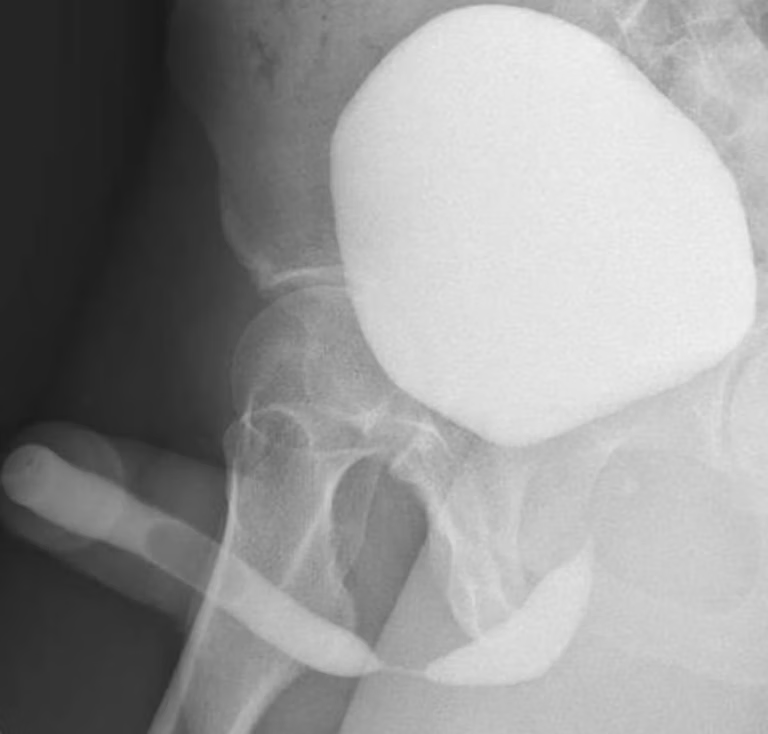
Radiographic appearance of a bulbar urethral stricture on RUG/VCUG: visible narrowing of the urethral lumen at the bulbar segment.
CT urethrography is an advanced imaging test that provides a detailed assessment of the urethra and surrounding structures, particularly in complex strictures or when surgery is planned. You lie on the CT table while a contrast agent is injected into a vein to make the bladder and urethra visible. When you feel the urge to urinate, you are asked to void into a dedicated device while remaining in position. Images are acquired during voiding to analyze urine flow through the urethra. This examination helps determine the exact location, length, and severity of the stricture, visualize the urethra within its anatomical environment (bones, prostate, bladder), detect associated abnormalities, and assist in planning tailored treatment.
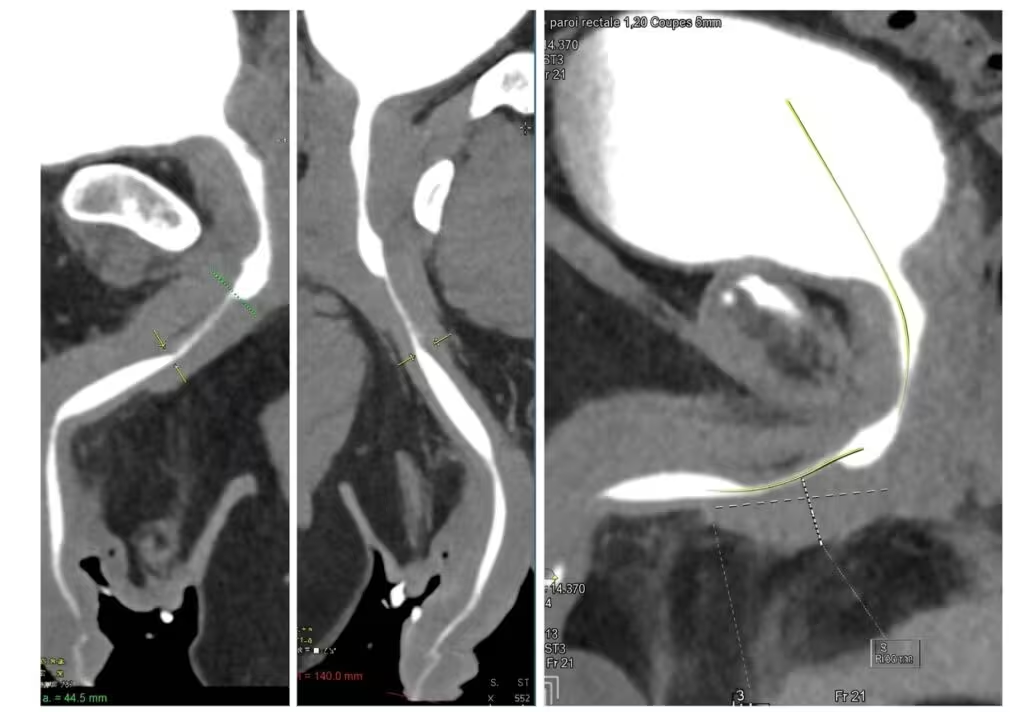

CT urethrography showing a long bulbar urethral stricture: visualization of an extended narrowing of the urethral lumen at the bulbar segment, with progressive tapering of the canal.
MR urethrography is a high-resolution imaging test that allows detailed visualization of the urethra and surrounding tissues. It is particularly useful in complex strictures, especially after pelvic trauma, prostate cancer treatment, or prior surgical failure. You lie on your back in the MRI scanner. To improve visualization, a sterile gel or saline is gently instilled into the urethra using a small catheter. This examination helps assess the length of the stricture, the condition of the urethral wall, and detect associated abnormalities such as fibrosis, fistula, or inflammation. It is often used in addition to other investigations.-
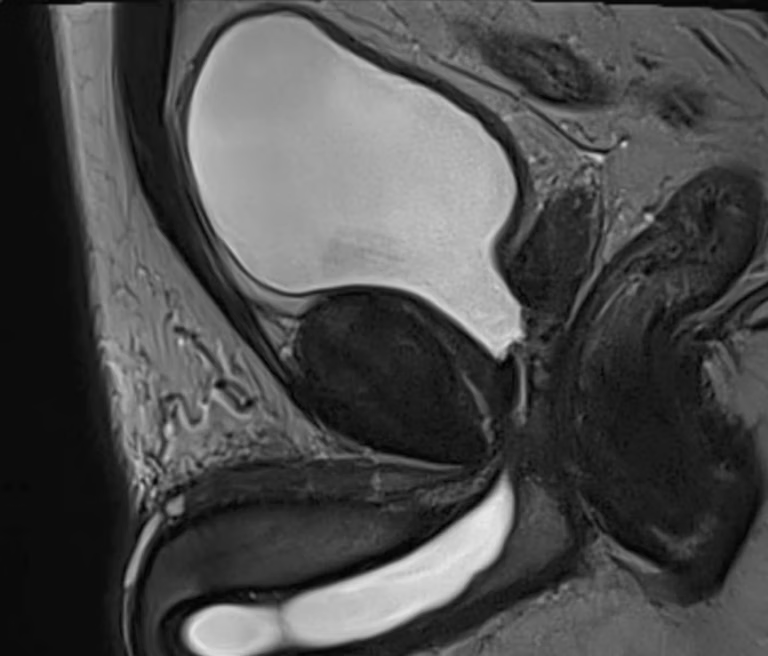
MR urethrography demonstrating a posterior urethral stenosis involving the prostatomembranous urethra.

Conclusion
A thorough evaluation combining symptoms, clinical examination, and imaging is essential to accurately diagnose urethral stricture and define its characteristics. This step ensures an individualized treatment strategy tailored to each patient’s condition and expectations.