Complex & Redo Cases
At URETRE PARIS, we manage some of the most difficult cases of urethral stricture disease, complex urethral reconstruction, posterior urethral stenosis, penile reconstruction, failed hypospadias repair, lichen sclerosus urethral disease Redo urethroplasty, pelvic fracture urethral injury, post-prostate treatment stenosis, rectourethral fistula, intersex genital reconstruction, exstrophy-epispadias, micropenis, acquired penile shortening, and urethral complications after phalloplasty.
These conditions usually require advanced reconstructive expertise, individualized planning, and a comprehensive approach addressing urinary function, sexual function, tissue quality, and overall reconstructive goals. In most cases, such situations are best managed in expert centers specialized in urethral and penile reconstruction.
Hypospadias Repair in Adults: Complex Urethral Strictures and Reconstruction
Video presentation of urethral strictures after hypospadias repair in adults
Urethral strictures after hypospadias repair in adults are among the most complex forms of urethral stricture disease. Often called failed hypospadias repair or crippled hypospadias, they may appear many years after childhood surgery.
These strictures are usually long and may involve part or all of the reconstructed urethra. They are frequently associated with lichen sclerosus, poor tissue quality, and a high risk of recurrence. Other common problems include urethrocutaneous fistula, penile curvature (chordee), and ventral skin deficiency, which may affect urination, sexual function, and cosmetic appearance.
Management must therefore be comprehensive and personalized. It should address urinary symptoms, penile shape, tissue loss, and overall reconstructive goals.
In this setting, endoscopic treatments such as dilation or internal urethrotomy are not effective. The standard treatment is urethroplasty, often using buccal mucosal grafts, staged reconstruction, or other advanced penile reconstructive techniques. In complex cases, more than one operation may be necessary to obtain a durable result.
These patients should ideally be treated in an expert center with experience in complex urethral reconstruction.
Lichen sclerosus, also known as balanitis xerotica obliterans (BXO), is a chronic inflammatory disease affecting the genital skin and urethra. It is one of the main causes of long and complex urethral strictures, especially panurethral stricture, in which a large part of the urinary channel becomes diseased.
When lichen sclerosus involves the urethra, the tissue becomes white, scarred, fragile, and unhealthy. The disease often extends beyond the urethra and also affects the glans and penile skin. This is important in reconstruction, because penile skin flaps are usually not recommended when the penile skin itself may also be affected by the disease.
In this setting, endoscopic treatments such as dilation or internal urethrotomy have no role. Repeated instrumentation may worsen the disease through the Koebner phenomenon, in which local trauma promotes new inflammatory lesions and additional scarring.
For this reason, urethral strictures caused by lichen sclerosus / BXO should be treated only by urethroplasty with replacement of the diseased urethral lining, most commonly using a buccal mucosal graft. Depending on the extent and severity of the stricture, reconstruction may be performed in one stage or two stages.
Redo urethroplasty after failed urethroplasty
Redo urethroplasty refers to reconstructive surgery performed after failure of a previous urethroplasty. These complex cases require a tailored approach, as prior surgery often leads to increased fibrosis, altered anatomy, and reduced tissue quality. Management depends on the location, extent, and complexity of the recurrent urethral stricture, as well as the techniques previously used, the patient’s overall condition, and the expected outcome. Advanced reconstructive options may include repeat anastomotic repair, augmentation urethroplasty using buccal mucosal grafts, or staged reconstruction. In selected cases, perineal urethrostomy may be considered.
However, redo urethroplasty is still the gold standard technique for recurrent stricture after a first urethroplasty, with high success rates, although these may be slightly lower than after a first attempt.
Pelvic Fracture Urethral Injury (PFUI)
Posterior urethral injury associated with pelvic fracture (PFUI) is a severe form of urethral trauma that occurs after high-energy accidents, usually in polytrauma patients. In the acute setting, the priority is always resuscitation and hemodynamic stabilization. Urethral treatment is not the first emergency, and urinary drainage is most often achieved with a suprapubic catheter.
Definitive treatment is usually delayed for several months and consists of posterior urethroplasty, most commonly excision and primary anastomosis through a perineal approach. This delayed reconstruction remains the gold-standard treatment and provides very high long-term success rates. Because these injuries are anatomically complex and may also affect continence and erectile function, PFUI should be managed in centers experienced in posterior urethral trauma and reconstructive surgery.

Principles of excision and primary anastomosis for posterior urethral disruption after pelvic fracture: these steps include isolated urethral mobilization, separation of the corporal crura, and, when necessary, inferior pubectomy, in order to shorten the bulbomembranous urethral curve as much as possible and achieve a tension-free anastomosis.
Posterior urethral stricture and stenosis after prostate treatment
After treatment for benign prostatic hyperplasia (BPH), specific bladder neck contractures may occur, especially after repeated endoscopic procedures. These stenoses affect the bladder outlet and are distinct from anterior urethral strictures. After failure of repeated endoscopic treatment, reconstructive surgery may be required. This is mainly performed using a robot-assisted approach, with techniques such as Y-V plasty, excision and re-anastomosis, or augmentation reconstruction using buccal mucosal grafts. The aim is not only to restore bladder outlet patency, but also to preserve sphincter function and urinary continence whenever possible.
Urethral narrowing can occur after prostate cancer treatment, including radical prostatectomy, radiotherapy, or ablative therapies such as HIFU or cryotherapy. These strictures typically affect the posterior urethra, involving the vesicourethral anastomosis (VUAS), the bladder neck, or sometimes the entire prostatic urethra. These are highly variable and complex cases, ranging from a short isolated narrowing to extensive posterior fibrosis after multimodal treatment. Tissue quality is often poor, especially after radiation, and surgical planning must take into account the anatomy of the stenosis, prior treatments, continence status, and overall bladder function. In selected early cases, endoscopic treatment may be attempted, but repeated failure or severe stenosis usually requires reconstructive surgery. Depending on the situation, treatment may include redo anastomosis, augmentation urethroplasty with buccal mucosal graft, or combined abdominal and perineal reconstruction. In the most severe cases, when reconstruction is not feasible because of extensive fibrosis, poor bladder function, or associated complications, urinary diversion may be required.
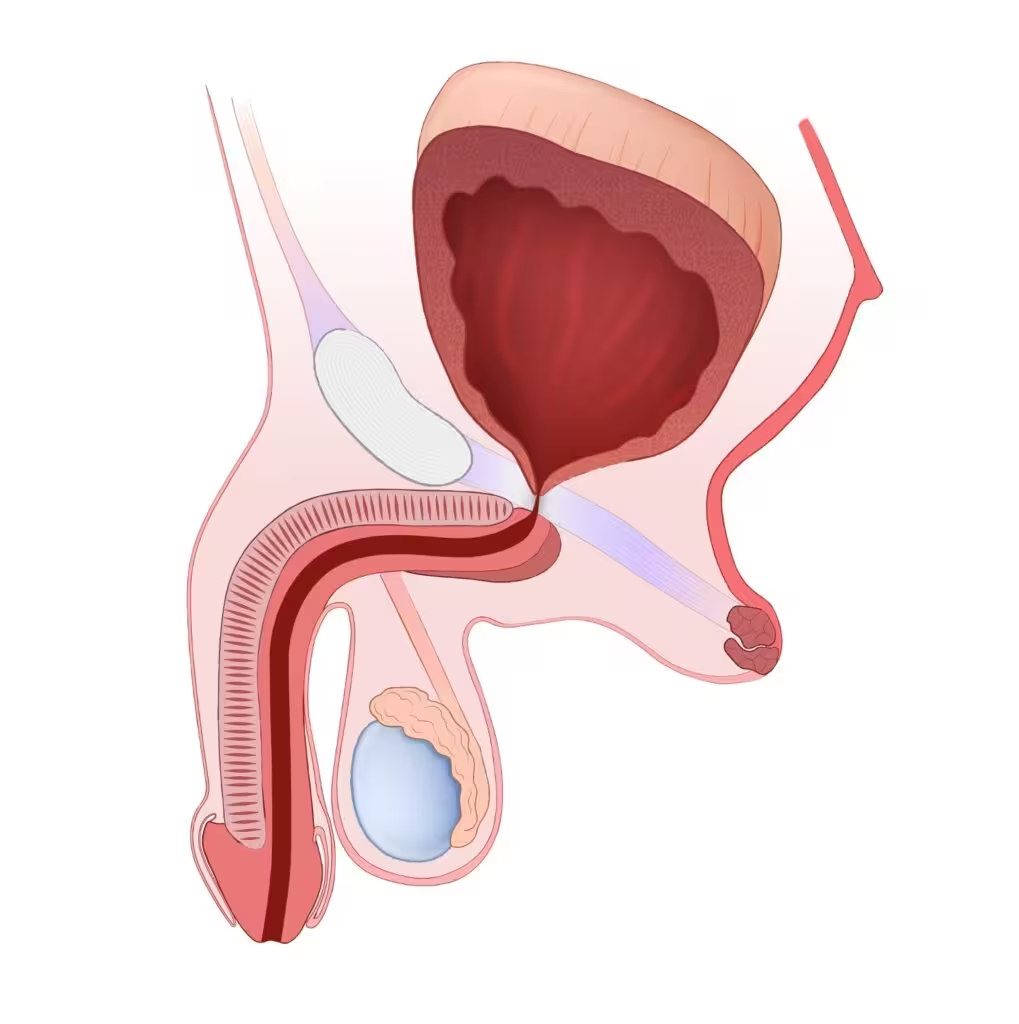
Post-Prostatectomy Vesicourethral Anastomotic Stenosis (VUAS) after Prostate Cancer Surgery
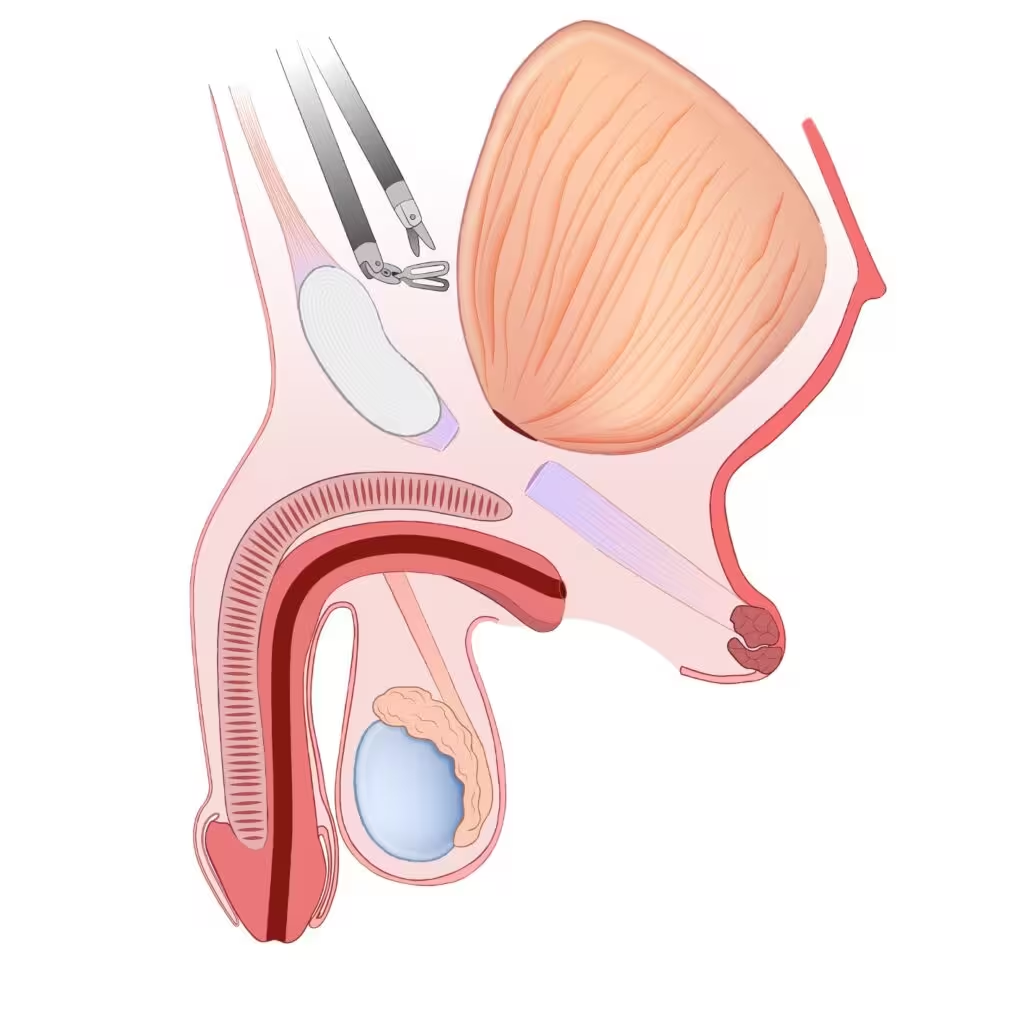
Combined Perineal and Robotic Mobilization of Vesicourethral Anastomotic Stenosis (VUAS)
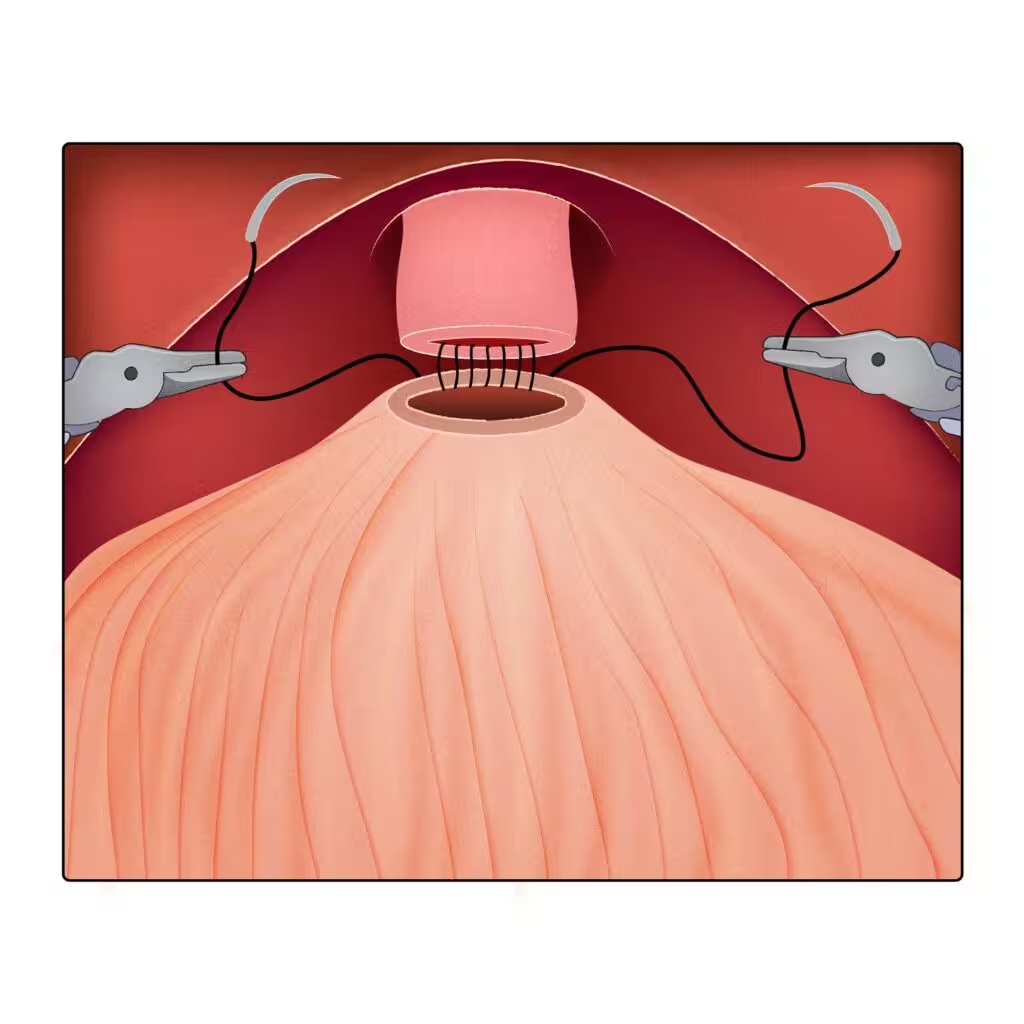
Robot-assisted redo vesicourethral anastomosis after excision of VUAS
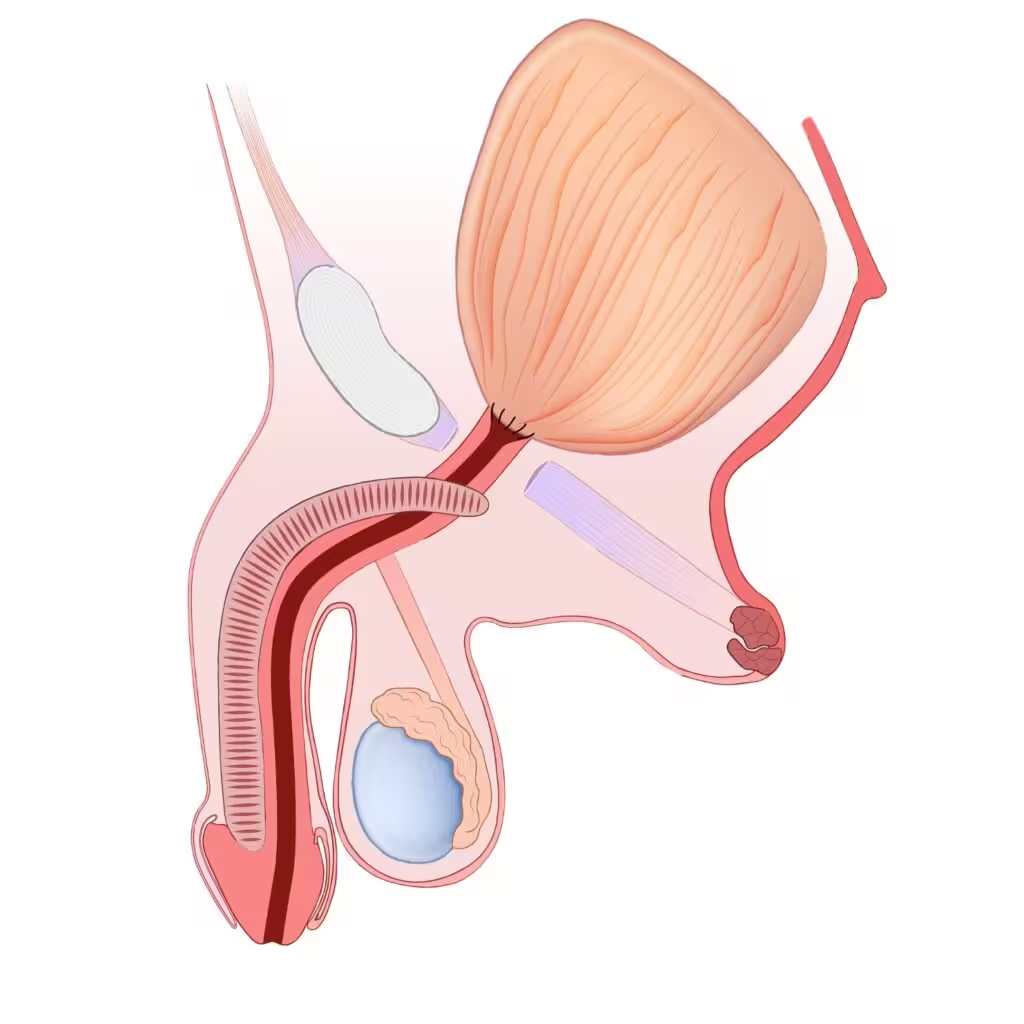
Final appearance after treatment of vesicourethral anastomotic stenosis using a combined perineal and transperitoneal robot-assisted approach: the MADEC technique

Rectourethral Fistula After Prostate Cancer Treatment
Rectourethral fistulas are rare but severe complications that may occur after prostate cancer treatment, particularly following surgery, radiotherapy, or combined therapies. These complex conditions create an abnormal connection between the urinary tract and the rectum, requiring specialized management.
One of the main reconstructive options is transperineal repair with gracilis muscle flap interposition. This technique allows closure of the fistula while providing well-vascularized tissue between the urethra and rectum to promote healing.
Success rates are around 90%, but outcomes depend on factors such as prior radiation, tissue quality, and patient comorbidities. These complex cases should be managed in an expert center with experience in urethral reconstruction and fistula repair.
Surgical video of rectourethral fistula repair using a gracilis muscle flap
Rectourethral fistula after prostate cancer treatment
Rectourethral fistula repair using a gracilis muscle flap

Intersex Conditions, Exstrophy-Epispadias, Micropenis, and Acquired Penile Shortening
At URETRE Paris, we offer the full spectrum of penile and urethral reconstruction, from conservative tissue-preserving procedures to the most advanced phallic reconstruction techniques. Our expertise includes urethral reconstruction, buried penis repair, penile straightening, correction of penile curvature, penile lengthening procedures, penile implants, and advanced genital reconstruction. Whenever possible, the goal is to preserve native tissues, restore urinary and sexual function, and improve penile shape and length. In the most severe situations or failed prior reconstruction, total phallic reconstruction may also be proposed. Each treatment plan is tailored to the patient’s anatomy, function, surgical history, and goals.
Urethral stricture is one of the most frequent complications after total phallic reconstruction, especially after phalloplasty with urethral lengthening. These strictures may affect different parts of the reconstructed urinary channel and are often associated with urethral fistulas or prior multiple surgeries. Management is complex and depends on the location, length, tissue quality, and type of genital reconstruction previously performed. In these challenging situations, staged urethroplasty is often the most reliable option, particularly for long or recurrent strictures. Treatment should be individualized and performed in an expert center with experience in urethral reconstruction after phalloplasty and masculinizing genital surgery.
Managing the most complex cases in urethral reconstruction at an expert referral center
Complex urethral disease often requires advanced reconstructive expertise and multidisciplinary decision-making. URETRE PARIS actively participates in dedicated multidisciplinary meetings focused on urethral stricture disease, named the CHARRUES meetings (Andrological, Reconstructive and Reparative Urethral Surgery Meetings) within the French Association of Urology. This approach ensures that patients benefit from expert, evidence-based diagnostic and therapeutic strategies for these highly complex situations.